


 216.73.216.110
216.73.216.110 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 216.73.xxx.xxx
216.73.xxx.xxx
 Server Time:
Server Time:
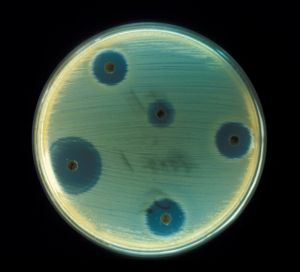
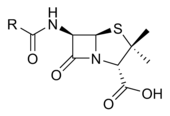
An antibiotic is a drug that kills or slows the growth of bacteria. They have no effect against viruses, fungi, or parasites. Antibiotics are one class of antimicrobials, a larger group which also includes anti-viral, anti-fungal, and anti-parasitic drugs. They are relatively harmless to the host, and therefore can be used to treat infections. The term, coined by Selman Waksman, originally described only those formulations derived from living organisms, in contrast to "chemotherapeutic agents", which are purely synthetic. Nowadays the term "antibiotic" is also applied to synthetic antimicrobials, such as the sulfa drugs. Antibiotics are generally small molecules with a molecular weight less than 2000. They are not enzymes. Some antibiotics have been derived from mold, for example the penicillin class.
Unlike previous treatments for infections, which included poisons such as strychnine and arsenic, antibiotics were labelled "magic bullets": drugs which targeted disease without harming the host. Conventional antibiotics are not effective in viral, fungal and other nonbacterial infections, and individual antibiotics vary widely in their effectiveness on various types of bacteria. Antibiotics can be categorised based on their target specificity: 'narrow-spectrum' antibiotics target particular types of bacteria, such as Gram-negative or Gram-positive bacteria, while 'wide-spectrum' antibiotics affect a larger range of bacteria.
The effectiveness of individual antibiotics varies with the location of the infection, the ability of the antibiotic to reach the site of infection, and the ability of the bacteria to resist or inactivate the antibiotic. Some antibiotics actually kill the bacteria (bactericidal), whereas others merely prevent the bacteria from multiplying (bacteriostatic) so that the host's immune system can overcome them.
Oral antibiotics are the simplest approach when effective, with intravenous antibiotics reserved for more serious cases. Antibiotics may sometimes be administered topically, as with eyedrops or ointments.
Antibiotics can also be classified by the organisms against which they are effective, and by the type of infection in which they are useful, which depends on the sensitivities of the organisms that most commonly cause the infection and the concentration of antibiotic obtainable in the affected tissue.
Contents |
History
Many ancient cultures, including the ancient Egyptians, ancient Greeks and ancient Chinese, already used moulds and plants to treat infections. This worked because some moulds produce antibiotic substances. However, they couldn't distinguish or distil the active component in the moulds.
Modern research on antibiotics began in Britain with the discovery of Penicillin in 1928 by Alexander Fleming. More than ten years later, Ernst Chain and Howard Florey became interested in his work, and came up with the purified form of penicillin. The three shared the 1945 Nobel Prize in Medicine. "Antibiotic" was originally used to refer only to substances extracted from a fungus or other microorganism, but has come to include also the many synthetic and semi-synthetic drugs that have antibacterial effects.
Classes of antibiotics
At the highest level, antibiotics can be classified as either bactericidal or bacteriostatic. Bactericidals kill bacteria directly where bacteriostatics prevent them dividing. However, these classifications are based on laboratory behaviour; in practice, both of these will end a bacterial infection.
| Class | Generic Name | Brand Names | Common Uses | Side Effects | |
|---|---|---|---|---|---|
| Aminoglycosides | |||||
| Amikacin | Amikin | Infections caused by Gram-negative bacteria, such as Escherichia coli and Klebsiella |
Hearing loss Vertigo Kidney damage |
||
| Gentamicin | Garamycin | ||||
| Kanamycin | |||||
| Neomycin | |||||
| Netilmicin | |||||
| Streptomycin | |||||
| Tobramycin | Nebcin | ||||
| Carbacephem | |||||
| Loracarbef | Lorabid | ||||
| Carbapenems | |||||
| Ertapenem | |||||
| Imipenem/Cilastatin | Primaxin | ||||
| Meropenem | |||||
| Cephalosporins (First generation) | |||||
| Cefadroxil | Duricef |
Gastrointestinal upset and diarrhea Nausea (if alcohol taken concurrently) Allergic reactions |
|||
| Cefazolin | Ancef | ||||
| Cephalexin | Keflex | ||||
| Cephalosporins (Second generation) | |||||
| Cefaclor | Ceclor |
Gastrointestinal upset and diarrhea Nausea (if alcohol taken concurrently) Allergic reactions |
|||
| Cefamandole | Mandole | ||||
| Cefoxitin | |||||
| Cefprozil | Cefzil | ||||
| Cefuroxime | Ceftin | ||||
| Cephalosporins (Third generation) | |||||
| Cefixime |
Gastrointestinal upset and diarrhea Nausea (if alcohol taken concurrently) Allergic reactions |
||||
| Cefdinir | Omnicef | ||||
| Cefditoren | |||||
| Cefoperazone | Cefobid | ||||
| Cefotaxime | Claforan | ||||
| Cefpodoxime | |||||
| Ceftazidime | Fortum | ||||
| Ceftibuten | |||||
| Ceftizoxime | |||||
| Ceftriaxone | Rocephin | ||||
| Cephalosporins (Fourth generation) | |||||
| Cefepime | Maxipime |
Gastrointestinal upset and diarrhea Nausea (if alcohol taken concurrently) Allergic reactions |
|||
| Glycopeptides | |||||
| Teicoplanin | |||||
| Vancomycin | Vancocin | ||||
| Macrolides | |||||
| Azithromycin |
Zithromax, Sumamed |
Streptococcal infections, syphilis, respiratory infections, mycoplasmal infections, Lyme disease |
Nausea, vomiting, and diarrhea (especially at higher
doses) Jaundice |
||
| Clarithromycin | Biaxin | ||||
| Dirithromycin | |||||
| Erythromycin | |||||
| Roxithromycin | |||||
| Troleandomycin | |||||
| Monobactam | |||||
| Aztreonam | |||||
| Penicillins | |||||
| Amoxicillin | Novamox | Wide range of infections; penicillin used for streptococcal infections, syphilis, and Lyme disease |
Gastrointestinal upset and diarrhea Allergy with serious anaphylactic reactions Brain and kidney damage (rare) |
||
| Ampicillin | |||||
| Azlocillin | |||||
| Carbenicillin | |||||
| Cloxacillin | |||||
| Dicloxacillin | |||||
| Flucloxacillin | |||||
| Mezlocillin | |||||
| Nafcillin | |||||
| Penicillin | |||||
| Piperacillin | |||||
| Ticarcillin | |||||
| Polypeptides | |||||
| Bacitracin | Mupirocin | Eye, ear or bladder infections; usually applied directly to the eye or inhaled into the lungs; rarely given by injection | Kidney and nerve damage (when given by injection) | ||
| Colistin | |||||
| Polymyxin B | |||||
| Quinolones | |||||
| Ciprofloxacin | Ciproxin, Ciplox | Urinary tract infections, bacterial prostatitis, bacterial diarrhea, gonorrhea | Nausea (rare) | ||
| Enoxacin | |||||
| Gatifloxacin | Tequin | ||||
| Levofloxacin | Levaquin | ||||
| Lomefloxacin | |||||
| Moxifloxacin | Avelox | ||||
| Norfloxacin | |||||
| Ofloxacin | Ocuflox | ||||
| Trovafloxacin | Trovan | ||||
| Sulfonamides | |||||
| Mafenide | Urinary tract infections (except sulfacetamide and mafenide); mafenide is used topically for burns |
Nausea, vomiting, and diarrhea Allergy (including skin rashes) Crystals in urine Kidney failure Decrease in white blood cell count Sensitivity to sunlight |
|||
| Prontosil (archaic) | |||||
| Sulfacetamide | |||||
| Sulfamethizole | |||||
| Sulfanilimide (archaic) | |||||
| Sulfasalazine | |||||
| Sulfisoxazole | |||||
| Trimethoprim | |||||
| Trimethoprim-Sulfamethoxazole (Co-trimoxazole) (TMP-SMX) | Bactrim | ||||
| Tetracyclines | |||||
| Demeclocycline | Syphilis, chlamydial infections, Lyme disease, mycoplasmal infections, acne rickettsial infections |
Gastrointestinal upset Sensitivity to sunlight Staining of teeth Potential toxicity to mother and fetus during pregnancy |
|||
| Doxycycline | Vibramycin | ||||
| Minocycline | |||||
| Oxytetracycline | |||||
| Tetracycline | Sumycin | ||||
| Others | |||||
| Chloramphenicol | Chloromycetin | ||||
| Clindamycin | Cleocin | ||||
| Ethambutol | |||||
| Fosfomycin | |||||
| Furazolidone | |||||
| Isoniazid | |||||
| Linezolid | Zyvox | ||||
| Metronidazole | Flagyl | ||||
| Nitrofurantoin | Macrodantin | ||||
| Platensimycin | |||||
| Pyrazinamide | |||||
| Quinupristin/Dalfopristin | Syncercide | ||||
| Rifampin | |||||
| Spectinomycin | |||||
| Class | Generic Name | Brand Names | Common Uses | Side Effects | |
Production
Since the first pioneering efforts of Florey and Chain in 1939, the importance of antibiotics to medicine has led to much research into discovering and producing them. The process of production usually involves screening of wide ranges of microorganisms, testing and modification. Production is carried out using fermentation; a process that is important in anaerobic conditions when there is no oxidative phosphorylation to maintain the production of ATP (Adenosine triphosphate) by glycolysis.
Side effects
Possible side effects are varied, and range from fever and nausea to major allergic reactions. One of the more common side effects is diarrhea, which results from the antibiotic disrupting the normal balance of intestinal flora, (which some people believe may be re-balanced by taking probiotics). Other side effects can result from interaction with other drugs, such as elevated risk of tendon damage from administration of a quinolone antibiotic with a systemic corticosteroid.
It is a common assertion that some antibiotics can interfere with the efficiency of birth control pills. Although there remain few known cases of complication, the majority of antibiotics do not interfere with oral contraception, despite widespread misinformation to the contrary.[2]
Antibiotic misuse
Common forms of antibiotic misuse include failure to take the entire prescribed course of the antibiotic, usually because the patient feels better, but before the infecting organism is completely eradicated. In addition to treatment failure, these practices can result in antibiotic resistance in which the bacteria survive the abbreviated treatment. Taking antibiotics in inappropriate situations is another common form of antibiotic misuse. Common examples of this would be the use of antibacterials for viral infections such as the common cold.
In the United States, vast quantities of certain antibiotics are routinely included as low doses in the diet of some kinds of healthy farm animals, where this practice has been shown to make animals grow faster. Opponents of this practice, however, point out the likelihood that it also leads to an environment conducive to the evolution of antibiotic resistance, frequently in bacteria that are known to also infect humans. There has been no convincing evidence yet that the evolution of antibiotic resistance in such bacteria is actually occurring. As the majority of bacteria is killed in the pasteurization process applied to the milk, and the cooking of the meat, of such animals, any possible resistance may go unnoticed until the bacteria survives it. Theoretically, though, there is a significant possibility that such resistances could be transferred through bacterial plasmids, and the aforementioned conditions of continuous, low-dose antibiotics are ideal for the development of antibiotic resistance.
Excessive use of prophylactic antibiotics in travelers may also be classified as misuse.
Antibiotic resistance
- Main article: Antibiotic resistance
Use or misuse of antibiotics may result in the development of antibiotic resistance by the infecting organisms, similar to the development of pesticide resistance in insects. Evolutionary theory of genetic selection requires that as close as possible to 100% of the infecting organisms be killed off to avoid selection of resistance; if a small subset of the population survives the treatment and is allowed to multiply, the average susceptibility of this new population to the compound will be much less than that of the original population, since they have descended from those few organisms which survived the original treatment. This survival often results from an inheritable resistance to the compound which was infrequent in the original population but is now much more frequent in the descendants thus selected entirely from those originally infrequent resistant organisms.

Antibiotic resistance has become a serious problem in both the developed and underdeveloped nations. By 1984 half of the people with active tuberculosis in the United States had a strain that resisted at least one antibiotic. In certain settings, such as hospitals and some child-care locations, the rate of antibiotic resistance is so high that the normal, low cost antibiotics are virtually useless for treatment of frequently seen infections. This leads to more frequent use of newer and more expensive compounds, which in turn leads inexorably to the rise of resistance to those drugs, and a never-ending ever-spiraling race to discover new and different antibiotics ensues, just to keep us from losing ground in the battle against infection. The fear is that we will eventually fail to keep up in this race, and the time when people did not fear life-threatening bacterial infections will be just a memory of a golden era.
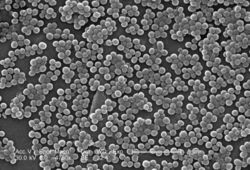
Another example of selection is Staphylococcus aureus, which could be treated successfully with penicillin in the 1940s and 1950s. At present, nearly all strains are resistant to penicillin, and many are resistant to nafcillin, leaving only a narrow selection of drugs such as vancomycin useful for treatment. The situation is worsened by the fact that genes coding for antibiotic resistance can be transferred between bacteria, making it possible for bacteria never exposed to an antibiotic to acquire resistance from those which have. The problem of antibiotic resistance is worsened when antibiotics are used to treat disorders in which they have no efficacy, such as the common cold or other viral complaints, and when they are used widely as prophylaxis rather than treatment (as in, for example, animal feeds), because this exposes more bacteria to selection for resistance.
Beyond antibiotics
Unfortunately, the comparative ease of finding compounds which safely cured bacterial infections proved much harder to duplicate with respect to fungal and viral infections. Antibiotic research led to great strides in our knowledge of basic biochemistry and to the current biological revolution; but in the process it was discovered that the susceptibility of bacteria to many compounds which are safe to humans is based upon significant differences between the cellular and molecular physiology of the bacterial cell and that of the mammalian cell. In contrast, despite the seemingly huge differences between fungi and humans, the basic biochemistries of the fungal cell and the mammalian cell are much more similar; so much so that there are few therapeutic opportunities for compounds to attack a fungal cell which will not harm a human cell. Similarly, we know now that viruses represent an incredibly minimal intracellular parasite, being stripped down to a few genes worth of DNA or RNA and the minimal molecular equipment needed to enter a cell and actually take over the machinery of the cell to produce new viruses. Thus, the great bulk of viral metabolic biochemistry is not merely similar to human biochemistry, it actually is human biochemistry, and the possible targets of antiviral compounds are restricted to the relatively very few components of the actual virus itself.
Research into bacteriophages is ongoing at the moment. Bacteriophages are a specific type of virus that only targets bacteria. Research suggests that nature has evolved several types of bacteriophage for each type of bacteria. While research into bacteriophages is only in its infancy the results are promising and have already lead to major advances in microscopic imaging.[3] While bacteriophages provide a possible solution to the problem of antibacterial resistance there is as of yet no proof that we will actually be able to deploy these microscopic killers in humans, we can only continue the research and see where it leads.
Phage therapy has been used in the past on humans in the US and Europe during the 1920s and 1930s, however due to not fully understanding the mechanism by which phage therapy worked, these treatments had mixed results. With the discovery of penicillin in the 1940s, Europe and the US changed to using antibiotics. However, in the former Soviet Union phage therapies continued to be studied. In the Republic of Georgia, the Eliava Institute of Bacteriophage, Microbiology & Virology continues to research the use of phage therapy. Various companies and foundations in North America and Europe are currently researching phage therapies.
References
- ^ The Merck Manual of Medical Information - Home Edition, Robert Berkow (Ed.), Pocket (September, 1999), ISBN 0-671-02727-1.
- ^ Planned Parenthood: Does taking antibiotics make the pill less effective?, July 15, 2004
- ^ Purdue University "Biologists build better software, beat path to viral knowledge", see Imaging of Epsilon 15, a virus that infects the bacterium Salmonella News report
External links
- Antibiotic News from Genome News Network (GNN)
- Bruce Sterling's Bitter Resistance
- JAAPA: New antibiotics useful in primary care
- A new method for controlling bacterial activity without antibiotics - Research conducted at the Hebrew University
