


 216.73.216.110
216.73.216.110 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 216.73.xxx.xxx
216.73.xxx.xxx
 Server Time:
Server Time:
Contents |
Clinical Use
These drugs are utilized in the treatment of many conditions such as:
- dyspepsia
peptic ulcer disease (PUD)
Zollinger-Ellison syndrome
gastroesophageal reflux disease (GORD/GERD)
prevention of stress gastritis
gastrinomas and other conditions that cause hypersecretion of acid
Mechanism of action
Proton pump inhibitors act by irreversibly blocking the hydrogen/potassium adenosine triphosphatase enzyme system (the H+/K+ ATPase, or more commonly just gastric proton pump) of the gastric parietal cell. The proton pump is the terminal stage in gastric acid secretion, being directly responsible for secreting H+ ions into the gastric lumen, making it an ideal target for inhibiting acid secretion.
Targeting the terminal-step in acid production, as well as the irreversible nature of the inhibition, result in a class of drugs that is significantly more effective than H2 antagonists and reduces gastric acid secretion by up to 99%.
The lack of the acid in the stomach will aid in the healing of duodenal ulcers, and reduces the pain from indigestion and heartburn, which is caused by excess stomach acid.
The proton pump inhibitors are given in an inactive form. The inactive form is neutrally charged (lipophilic) and readily crosses cell membranes into intracellular compartments (like the parietal cell canaliculus) that have acidic environments. In an acid environment, the inactive drug is protonated and rearranges into its active form. As described above, the active form will covalently and irreversibly bind to the gastric proton pump, deactivating it.
Pharmacokinetics
Generally, the absorption of proton pump inhibitors is unaffected by co-administration with food. The rate of omeprazole absorption, however, is decreased by concomitant food intake. Additionally, the absorption of lansoprazole and esomeprazole is decreased and delayed by food. These pharmacokinetic effects, however, reportedly have no significant impact on efficacy (Wyeth Australia, 2004; AstraZeneca, 2005).
The elimination half-life of proton pump inhibitors ranges from 0.52 hours, however the effect of a single dose on acid secretion usually persists up to 23 days. This is because of accumulation of the drug in parietal cell canaliculi and the irreversible nature of proton pump inhibition.
Examples of proton pump inhibitors
Clinically used proton pump inhibitors:
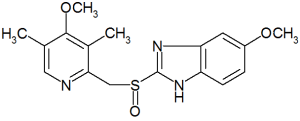
- Omeprazole (brand names: Losec®, Prilosec®)
- Lansoprazole (brand names: Prevacid®, Zoton®, Inhibitol®)
- Esomeprazole (brand names: Nexium®)
- Pantoprazole (brand names: Protonix®, Somac®,
Pantoloc®)
Rabeprazole (brand names: Rabecid®, Aciphex®, Pariet®)
Adverse effects
Proton pump inhibitors are generally well tolerated, and the incidence of adverse effects is relatively uncommon. The range and occurrence of adverse effects are similar for all of the proton pump inhibitors, though they have been reported more frequently with omeprazole. This may be due to its longer availability and hence clinical experience.
Common adverse effects include: headache, nausea, diarrhoea, abdominal pain, fatigue, dizziness. (Rossi, 2004)
Infrequent adverse effects include: rash, itch, flatulence, constipation. Decreased cyanocobalamin (vitamin B12) absorption may occur with long-term use (Rossi, 2006).
Recently it has been observed that gastric acid suppression, using H2-receptor antagonists and proton pump inhibitors, is associated with an increased risk of community-acquired pneumonia. It is suspected that acid suppression results in insufficient elimination of pathogenic organisms. It has therefore been suggested that patients at higher risk of pneumonia should only be prescribed proton pump inhibitors at lower doses and only when necessary. (Laheij et al., 2004).
PPIs have been shown to raise risk of C. difficile infection [1]
References
- AstraZeneca Pty Ltd. Nexium (Australian approved prescribing information). North Ryde: AstraZeneca; 2005.
- Katzung, BG. Basic & clinical pharmacology, 9th edition. New York : Lange Medical Books; 2004. ISBN 0-07-141092-9
- Rossi S, editor. Australian Medicines Handbook 2006. Adelaide: Australian Medicines Handbook; 2006. ISBN 0-9757919-2-3
- Laheij RJF, Sturkenboom MCJM, Hassing R-J, Dieleman J, Stricker BHC, Jansen JBMJ. Risk of community-acquired pneumonia and use of gastric acid-suppressive drugs. JAMA 2004;292(16): 1955-60. PMID 15507580
- Wyeth Australia Pty Ltd. Zoton (Australian approved prescribing information). Baulkham Hills: Wyeth; 2004.
- PPIs raise risk of C. difficile infection
