


 216.73.216.133
216.73.216.133 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 216.73.xxx.xxx
216.73.xxx.xxx
 Server Time:
Server Time:
 |
|
 |
|
|
Methylphenidate
|
|
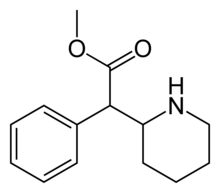
| Systematic (IUPAC) name | |
| methyl 2-phenyl-2-(2-piperidyl)acetate | |
| Identifiers | |
| CAS number | 113-45-1 |
| ATC code | N06BA04 |
| PubChem | 4158 |
| DrugBank | APRD00657 |
| Chemical data | |
| Formula | C14H19NO2 |
| Mol. weight | 233.306 g/mol |
| Pharmacokinetic data | |
| Bioavailability | 1152% |
| Metabolism | Liver |
| Half life | 24 hours |
| Excretion | Urine |
| Therapeutic considerations | |
| Pregnancy cat. | C |
| Legal status | Class B(UK) Schedule II(US) |
| Indicated for: ADD Recreational uses: Stimulant / "Speed" / "Uppers" Other uses: treatment-resistant depression antidepressant augmentation |
|
Contraindications: Use of tricyclic antidepressants (e.g. desipramine), as MPH may dangerously increase their plasma concentrations, leading to potential toxic reactions (mainly, cardiovascular effects). Use of MAO Inhibitors, such as phenelzine (Nardil) or tranylcypromine (Parnate), and certain other drugs. MPH should not be given to patients who suffer from the following conditions: Severe Arrhythmia, Hypertension or Liver damage. Drug-seeking behaviour Pronounced agitation or nervousness |
|
Side effects:
Cardiovascular: Tachycardia Endocrinal: Appetite loss Eye: Blurred vision Pupil dilation (If snorted) Gastrointestinal: Nausea/vomiting, abdominal pain Musculoskeletal: Muscle twitches Neurological: Insomnia, drowsiness, dizziness, headache Psychological: Nervousness Respiratory: Increased respiration rate |
Methylphenidate (MPH) is an amphetamine-like prescription stimulant commonly used to treat Attention Deficit Hyperactivity Disorder (ADHD) in children and adults. It is also one of the primary drugs used to treat symptoms of traumatic brain injury and the daytime drowsiness symptoms of narcolepsy and chronic fatigue syndrome. Brand names of drugs that contain methylphenidate include Ritalin® (Ritalina®, Rilatine®), Attenta®, Concerta® (a timed-release capsule), Metadate®, Methylin® and Rubifen®. Focalin® is a preparation containing only dextro-methylphenidate, rather than the usual racemic dextro- and laevo-methylphenidate mixture of other formulations.
Contents |
History
Methylphenidate was patented in 1954 by the Ciba pharmaceutical company (one of the predecessors of Novartis) and was initially prescribed as a treatment for depression, chronic fatigue, and narcolepsy, among other ailments. Beginning in the 1960s, it was used to treat children with ADHD, known at the time as hyperactivity or minimal brain dysfunction (MBD). Today methylphenidate is the medication most commonly prescribed to treat ADHD around the world. According to most estimates, more than 75 percent of methylphenidate prescriptions are written for children, with boys being about four times as likely to take methylphenidate than girls. Production and prescription of methylphenidate rose significantly in the 1990s, especially in the United States, as the ADHD diagnosis came to be better understood and more generally accepted within the medical and mental health communities. Methylphenidate has been used illegally by students for whom the drug has not been prescribed, to assist with coursework and examinations. [1]
While ADHD medication is directed for children, it has not been studied for children under the age of 6. It is also important to note that while ADHD is a condition that includes hyperactivity, problems holding still, and following directions, this is also typical of a child under the age of 6. This causes difficulty in diagnosing children under this age and should probably not be studied.[1]
Most brand-name Ritalin is produced in the United States, although methylphenidate is also produced in Mexico and Argentina by respective contract pharmaceutical manufacturers and is most commonly marketed under the brand name "Ritalin" for Novartis. In the United States, various generic forms of methylphenidate are also produced by several pharmaceutical companies (such as Methylin, etc.), and Ritalin is also sold in the United Kingdom, Germany, and other European countries (although in much lower volumes than the United States). These generic versions of methylphenidate tend to outsell brand-name "Ritalin" four-to-one. In Belgium the product is sold under the name "Rilatine" for Novartis.
Another medicine is Concerta, a once-daily extended release form of methylphenidate, which was approved in April 2000. Studies have demonstrated that long-acting methylphenidate preparations such as Concerta are just as effective, if not more effective, than IR (instant release) formulas. [2] [3] [4] [5] Time-release medications are also harder to misuse.
In April 2006, the FDA approved a transdermal patch for the treatment of ADHD, called Daytrana. The once-daily patch administers methylphenidate in doses of 10, 15, 20, or 30mg.[6] However, the patch must be applied several hours before the effect is desired, and the drug's effect remains for several hours after removal, making it necessary to remove the patch in the mid-to-late afternoon or else insomnia may result.
Effects
Methylphenidate is a central nervous system (CNS) stimulant. It is claimed to have a 'calming' effect on many children who have ADHD,[7] reducing impulsive behavior and the tendency to "act out", and helps them concentrate on schoolwork and other tasks. Adults who have ADHD often claim that MPH increases their ability to focus on tasks and organize their lives.
Methylphenidate has been found to have a lower incidence of side-effects compared to dextroamphetamine, a less commonly prescribed medication. [8] When prescribed at the correct dosage, methylphenidate is usually well-tolerated by patients.[2]
The means by which methylphenidate helps people with ADHD are not well understood. Some researchers have theorized that ADHD is caused by a dopamine imbalance in the brains of those affected. MPH is a dopamine reuptake inhibitor, which means that it increases the level of the dopamine neurotransmitter in the brain by partially blocking the transporters that remove it from the synapses. [9] An alternate explanation which has been explored is that the MPH affects the action of serotonin in the brain.[10]
In the United States, methylphenidate is classified as a Schedule II controlled substance, the designation used for substances that have a recognized medical value but which have a high potential for abuse because of their addictive potential. Internationally, methylphenidate is a Schedule II drug under the Convention on Psychotropic Substances. [11] Some people abuse MPH by crushing the tablets and snorting them, the "high" resulting from the increased rate of dopamine transporter blockade due to quicker absorption into the bloodstream. In this manner, the effect of Ritalin is similar to that of cocaine or amphetamine and such abuse can lead to addiction. When taken orally in prescribed doses, MPH has a low addiction liability and rarely produces a "high".
Side effects
Common reported side effects are[12][13]: difficulty sleeping (which can lead in turn to other problems); loss of appetite (thus its use as an appetite suppressant); Depression; irritability; nervousness; stomach aches; headaches; dry mouth; blurry vision; nausea; dizziness; drowsiness; motor tics or tremors. Up to 5% of children experience disturbing hallucinations often involving worms, snakes, or insects (New Scientist, 31 March 2006).
Less common side effects are: hypersensitivity; anorexia; palpitations; blood pressure and pulse changes; cardiac arrhythmia; anemia; scalp hair loss; toxic psychosis.
There have also been reports of: abnormal liver function; cerebral arteritis; leukopenia; death. There have been at least 19 cases of sudden death in children taking methylphenidate, leading to calls by the Drug Safety and Risk Management Advisory Committee to the FDA to require the most serious type of health warning on the label, but this advice was rejected (New Scientist 18 Feb. 2006).
Medline [14] lists a number of side-effects of unquantified frequency.
Formulations
Most products containing methylphenidate contain a racemic mixture of dextro-methylphenidate and levo-methylphenidate, although it is only dextro-methylphenidate, the active enantiomer, which is considered to provide the pharmacologically useful effects of mental focus. However, with the introduction of Focalin, pure dextro-methylphenidate is available. Described as a fast-acting form of the drug, it is absorbed more quickly by the body, with a shorter time to peak concentration (and excretion) than with the racemic compound.
The pharmacological profiles and relative usefulness of dextro- and levo-methylphenidate is analogous to what is found in amphetamine, where dextro-amphetamine is considered to have a more beneficial effect than levo-amphetamine.
Delivery
Ritalin: 5 mg, 10 mg and 20 mg tablets;
Ritalin SR: 20 mg tablets;
Ritalin LA: 20 mg, 30 mg and 40 mg capsules;
Attenta: 10mg tablets;
Methylin: 5 mg, 10 mg, and 20 mg tablets;
Methylin ER: 10 mg and 20 mg tablets;
Metadate ER: 10 mg and 20 mg tablets;
Metadate CD: 10 mg, 20 mg and 30 mg capsules;
Concerta: 18 mg, 27 mg, 36 mg and 54 mg tablets;
Equasym: 5 mg, 10 mg tablets;
Rubifen: 5 mg, 10 mg and 20 mg tablets;
Daytrana: 10 mg, 15 mg, 20 mg, 30 mg and 40 mg
patches
Criticism
Similarity to Cocaine
Like cocaine, methylphenidate is a powerful stimulant that increases alertness and productivity. Methylphenidate and cocaine have similar chemical structures. [15] Their effects, too, are similar; both increase the brain-levels of dopamine -- a joy-inducing neurotransmitter -- by blocking the ability of neurons to reabsorb dopamine. When taken as prescribed, however, Methylphenidate is absorbed into the body at a much slower rate than cocaine. In this way, methylphenidate is like low-dosage, slow-acting cocaine. [16] The similarities between methylphenidate and cocaine have prompted concern that the unknown dangers of methylphenidate could be similar to the known dangers of cocaine. [17] There have also been some reports showing a cross-tolerance between cocaine, methylphenidate, and a third common stimulant, amphetamine. [18]
Overprescription
The incidence of ADHD is believed to be between three and five percent of the population, while the number of children in America taking Ritalin is estimated at one to two percent. [19] In a small study of four American communities, the incidence of ADHD varied from 1.6% to 9.4%. The study also found that 12.5% of the children meeting the DSM-III-RADHD criteria for ADHD had been treated with stimulants during the past year.[20]
Addiction
The question of whether or not MPH use in children leads to future addictive tendencies has sparked many inquiries and analyses. One study examined the history of a group of adults who had used cocaine at least once, and found that those who as children had been medically diagnosed with hyperactivity and had received methylphenidate treatment for between one and ten years had a percentage of cocaine abuse twice that of either of two control groups: one group of same-age individuals who had not been diagnosed with hyperactivity, and one group of individuals who had also been diagnosed with hyperactivity but had not been treated with stimulants. This research has been described as indicating that "... methylphenidate was still capable of explaining a small but significant proportion of the variance in cocaine use even after approximately 15 years."[21] On the flip side, a 2003 project suggests that boys with ADHD who are treated with stimulants like MPH are actually less likely to abuse drugs (including alcohol) later in life.[22]
Long-term effects
Ritalin has been used on a long-term basis since the mid-20th century, yet clinical studies of the long-term use effects have not been undertaken. A great deal of controversy has been generated by non-expert groups, many of them basing 'research' on the negative effects of ritalin on children. Many of these reports have been forwarded by Scientology-related groups.
In a 2005 study, no "clinically significant" effects on growth, vital signs, tics, or laboratory tests (including urinalysis, hematology/complete blood counts, electrolytes, and liver function tests) were observed after 2 years of treatment. [23]
Still, some theoretical studies raise theoretical questions. For example, Adriani et al (2005) found plastic changes in reward related behavior in rats after they were in a drug-free state. [24] Whether or not this would have any effect on human cognition is unknown.
Effects on stature
Researchers have also looked into the role of methylphenidate in affecting stature, with some studies finding slight decreases in height acceleration. [25] Other studies indicate height may normalize by adolescence. [26] [27]
Risk of death
As mentioned above, methylphenidate has been implicated in cases of sudden death by heart failure. The FDA decided against requiring warning labels, even though its advisory committee voted in favor of this. According to the Merck Index Methylphenidate had an LD50 of 150mg/kg body mass.
Potential Carcinogen
In February 2005, a team of researchers from The University of Texas M.D. Anderson Cancer Center led by R.A. El-Zein announced that a small scale study of 12 children indicated that methylphenidate may be carcinogenic. In the study, 12 children were given standard therapeutic doses of methylphenidate. At the conclusion of the 3 month study, all 12 children displayed significant, treatment induced chromosomal aberrations. The researchers indicated that while their study was relatively small, they indicated the results should be reproduced one more time in a bigger population for a definitive conclusion about the genotoxicity of methylphenidate to be drawn. The link between chromosomal aberrations and cancer risk has been established. [28]
The results are controversial, however, since there have been conflicting results regarding the mutagenicity of methylphenidate.
A 2003 study tested the effects of d-methylphenidate (Focalin), l-methylphenidate, and d,l-methylphenidate (Ritalin) on mice to search for any carcinogenic effects. The researchers found that all three compounds were non-genotoxic and non-clastogenic; d-MPH, d,l-MPH, and l-MPH did not cause mutations or chromosome aberrations. They concluded that none of the compounds present a carcinogenic risk to humans. [29]
In 2005, the U.S. Food and Drug Administration issued a series of public health advisories warning that Ritalin and its sister drugs may cause visual hallucinations, suicidal thoughts, psychotic behavior, as well as agression or violent behavior.
Illicit use
Both the United States Drug Enforcement Administration (DEA) and the United Nations International Narcotics Control Board have expressed concern about the ease with which legally prescribed MPH is diverted to the illicit market.[30][31]
According to the DEA, "The increased use of this substance [MPH] for the treatment of ADHD has paralleled an increase in its abuse among adolescents and young adults who crush these tablets and snort the powder to get high. Youngsters have little difficulty obtaining methylphenidate from classmates or friends who have been prescribed it."[32]
Street names for Ritalin include: diet coke, kiddie cocaine, kiddie coke, vitamin R, R-ball, poor man's cocaine, rids, skittles, and smarties.
See also
- Phenethylamines
- Psychoactive drug
- Stimulant
- Amphetamine
- Methamphetamine
- Benzedrine
- Attention Deficit Disorder
Footnotes
- ^ Pittsburgh Tribune-Review. "More students abusing hyperactivity drugs".
- ^ a b Steele, M., et al. (2006). "A randomized, controlled effectiveness trail of OROS-methylphenidate compared to usual care with immediate-release methylphenidate in Attention Deficit-Hyperactivity Disorder". Can J Clin Pharmacol. 2006 Winter;13(1):e50-62.
- ^ Pelham, W.E., et al. (2001). "Once-a-day Concerta methylphenidate versus three-times-daily methylphenidate in laboratory and natural settings". Pediatrics. 2001 Jun;107(6):E105.
- ^ Keating, G.M., McClellan, K., Jarvis, B. (2001). "Methylphenidate (OROS formulation)". CNS Drugs. 2001;15(6):495-500; discussion 501-3.
- ^ Hoare, P., et al. (2005). "12-month efficacy and safety of OROS® MPH in children and adolescents with attention-deficit/hyperactivity disorder switched from MPH". Eur Child Adolesc Psychiatry. 2005 Sep;14(6):305-9.
- ^ Peck, P. (2006, 7 April). FDA Approves Daytrana Transdermal Patch for ADHD. MedPage today. Retrieved April 7, 2006, from http://www.medpagetoday.com/ProductAlert/Prescriptions/tb/3027.
- ^ Hyperactivity Paradox Resolved?. Journal Watch. Retrieved on 2006-11-11.
- ^ Barbaresi, W.J., et al. (2006). "Long-Term Stimulant Medication Treatment of Attention-Deficit/Hyperactivity Disorder: Results from a Population-Based Study". J Dev Behav Pediatr. 2006 Feb;27(1):1-10.
- ^ Volkow N., et al. (1998). "Dopamine Transporter Occupancies in the Human Brain Induced by Therapeutic Doses of Oral Methylphenidate". Am J Psychiatry 155:1325-1331, October 1998.
- ^ Gainetdinov, Raul R., Caron, Marc G. (March 2001). "Genetics of Childhood Disorders: XXIV. ADHD, Part 8: Hyperdopaminergic Mice as an Animal Model of ADHD". Journal of the American Academy of Child & Adolescent Psychiatry 40 (3): 380-382. Retrieved on 2006-11-11.
- ^ Green List: Annex to the annual statistical report on psychotropic substances (form P) 23rd edition. August 2003. International Narcotics Board, Vienna International Centre. Accessed 02 March 2006
- ^ MedicineNet
- ^ ADD ADHD Information
- ^ MedLine
- ^ http://www.biopsychiatry.com/methcomp.htm Is methylphenidate like cocaine? Studies on their pharmacokinetics and distribution in the human brain. Volkow ND, Ding YS, Fowler JS, Wang GJ, Logan J, gatley JS, Dewey S, Ashby C, Liebermann J, Hitzemann R, et al Medical Department, State University of New York, Stony Brook, USA, Arch Gen Psychiatry 1995 Jun; 52(6):456-63
- ^ http://www.biopsychiatry.com/methcomp.htm Is methylphenidate like cocaine? Studies on their pharmacokinetics and distribution in the human brain. Volkow ND, Ding YS, Fowler JS, Wang GJ, Logan J, gatley JS, Dewey S, Ashby C, Liebermann J, Hitzemann R, et al Medical Department, State University of New York, Stony Brook, USA, Arch Gen Psychiatry 1995 Jun; 52(6):456-63
- ^ http://www.slate.com/id/2076413/ Is Ritalin "Chemically Similar" to Cocaine? Brendan I. Koerner. Jan 6, 2003 Washingtonpost.Newsweek Interactive Co. LLC
- ^ http://www.springerlink.com/content/m4j5207r64367645/ Self-stimulation and amphetamine: Tolerance to d and l isomers and cross tolerance to cocaine and methylphenidate Nancy J. Lieth and Robert J. Barret. June 1981 Journal of Psychopharmacology
- ^ The New Yorker. 2 February 1999. "Running from Ritalin".
- ^ Jensen, Peter S., Lori Kettle, Margaret T. Roper, Michael T. Sloan, Mina K. Dulcan, Christina Hoven, Hector R. Bird, Jose J. Bauermeister, and Jennifer D. Payne. 1999. Are stimulants overprescribed? Treatment of ADHD in four U.S. communities. Journal of the American Academy of Child and Adolescent Psychiatry 38 (7):797-804.
- ^ Schenk, Susan and Davidson, Emily S.. Stimulant Preexposure Sensitizes Rats and Humans to the Rewarding Effects of Cocaine. NIDA Res Monogr. 1998 Mar;169:56-82
- ^ Mannuzza, S., Klein, R.G., Moulton, J.L. (2003). "Does Stimulant Treatment Place Children at Risk for Adult Substance Abuse? A Controlled, Prospective Follow-up Study". Journal of Child and Adolescent Psychopharmacology, Sep 2003, Vol. 13, No. 3: 273-282.
- ^ Wilens, T., et al. (2005). ADHD treatment with once-daily OROS methylphenidate: final results from a long-term open-label study". J Am Acad Child Adolesc Psychiatry. 2005 Oct;44(10):1015-23.
- ^ Adriani, W. et al. (2005). "Methylphenidate Administration to Adolescent Rats Determines Plastic Changes on Reward-Related Behavior and Striatal Gene Expression". Neuropsychopharmacology advance online publication 23 November 2005;doi:10.1038/sj.npp.1300962.
- ^ Rao J.K., Julius J.R., Breen T.J., Blethen S.L. (1996). "Response to growth hormone in attention deficit hyperactivity disorder: effects of methylphenidate and pemoline therapy". Pediatrics. 1998 Aug;102(2 Pt 3):497-500.
- ^ Spencer, T.J., et al. (1996). "Growth deficits in ADHD children revisited: evidence for disorder-associated growth delays?". J Am Acad Child Adolesc Psychiatry. 1996 Nov;35(11):1460-9.
- ^ Klein R.G. & Mannuzza S. (1988). "Hyperactive boys almost grown up. III. Methylphenidate effects on ultimate height". Arch Gen Psychiatry. 1988 Dec;45(12):1131-4.
- ^ El-Zein R.A., et al. (2005). "Cytogenetic effects in children treated with methylphenidate". Cancer Lett. 2005 Dec 18;230(2):284-91.
- ^ Teo, S.K., et al. (2003). "D-Methylphenidate is non-genotoxic in vitro and in vivo assays". Mutat Res. 2003 May 9;537(1):67-79.
- ^ United Nations International Narcotics Control Board. 1995. Dramatic Increase in Methylphenidater Consumption in US: Marketing Methods Questioned [Web page]. Author, [cited 19 April 2004]. Available from http://www.incb.org/e/press/1995/pdf/e_bn_02.pdf.
- ^ United States Drug Enforcement Administration. 2000. Statement by Terrance Woodworth Deputy Director, Office of Diversion Control, Drug Enforcement Administration Before the Committee on Education and the Workforce: Subcommittee on Early Childhood, Youth and Families May 16, 2000 [Web page], [cited 19 April 2004]. Available from http://www.usdoj.gov:80/dea/pubs/cngrtest/ct051600.htm.
- ^ DEA, Briefs & Backgrounds, Drugs and Drugs of Abuse, Descriptions, Methylphenidate. Retrieved April 7, 2006 from http://www.usdoj.gov/dea/concern/methylphenidate.html.
External links
- Ritalin(R) 10mg Consumer Medicine Information (Australia)
- Erowid Methylphenidate Vault
- Information from the manufacturer on the methylphenidate ADHD Patch
- U.S. Drug Enforcement Administration statement on MPH abuse
- Dep't of Energy 1998 Sep 29 press release on Ritalin
- CBS: Kiddie Cocaine
- Children and Medication - a multimodal presentation
- Website of anti-Ritalin advocate Dr. Peter Breggin see the Wikipedia article on Peter Breggin
- Students without ADHD are using Ritalin to help them study
- Why I Believe that Attention Deficit Disorder is a Myth
- Is methylphenidate like cocaine?
- Methylphenidate and cocaine have a similar in vivo potency to block dopamine transporters in the human brain
- Dexmethylphenidate
