


 216.73.216.110
216.73.216.110 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 216.73.xxx.xxx
216.73.xxx.xxx
 Server Time:
Server Time:
 |
|
|
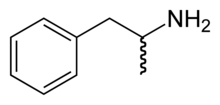
Amphetamine
|
|
| Systematic (IUPAC) name | |
| 1-phenylpropan-2-amine | |
| Identifiers | |
| CAS number | 300-62-9 |
| ATC code | N06BA01 |
| PubChem | 3007 |
| DrugBank | APRD00480 |
| Chemical data | |
| Formula | C9H13N |
| Mol. weight | 135.2084 |
| Pharmacokinetic data | |
| Bioavailability | 4L/kg; low binding to plasma proteins (20%) |
| Metabolism | Hepatic |
| Half life | 1013 hours |
| Excretion | Renal; significant portion unaltered |
| Therapeutic considerations | |
| Pregnancy cat. | C (USA) |
| Legal status |
DEA Schedule II (USA) Class B (UK) Schedule III (Canada) |
| Routes | Oral, Intravenous, Vaporized, Insufflated, Suppository |
Amphetamine (alpha-methyl-phenethylamine), also known as speed or crank, is a stimulant, and club drug, used to diminish the appetite, control weight, and treat disorders including narcolepsy and attention-deficit hyperactivity disorder. It is also used recreationally and for performance enhancement (these uses are illegal in some countries).
Illicit production and use of amphetamines occurs on a widescale basis in several European nations, typically in the form of amphetamine sulfate synthesized from phenylpropanolamine. In addition, because of the widespread use of amphetamines as a treatment for narcolepsy and ADD/ADHD, prescription amphetamines are subject to diversion and are one of the most frequently-abused drugs in high schools and colleges.
Contents |
Toxicity
Patients with acute toxicity from amphetamines may have symptoms of psychosis, disorientation, temporary symptoms associated with schizophrenia, aggression, delusions, lock-jaw, diarrhea, palpitations, arrhythmia, syncope, hyperpyrexia, and hyperreflexia progressing to convulsions and coma. Patients with chronic use of amphetamines develop a rapid tolerance to the drug and may have to increase the dose to reach the desired effect and eventually develop addiction. Patients that develop addiction show symptoms of restlessness, anxiety, depression, insomnia, and suicidal behavior. A urine drug screen can be performed to determine the presence of amphetamines. Patients may need to be hospitalized. Supportive therapy is important. Cooling blankets may be used for hyperthermia. Sedation may be obtained with lorazepam or diazepam. Haloperidol may be given for agitation and delusions. Hypertension and arrhythmias should be treated.
Chemistry
Amphetamine was first synthesized in 1887 by the Romanian chemist Lazăr Edeleanu at the University of Berlin, who called it "phenylisopropylamine". Amphetamine is a chiral compound. The racemic mixture can be divided into its optical antipodes: levo- and dextro-amphetamine. Amphetamine is the parent compound of its own structural class, comprising a broad range of psychoactive derivatives, e.g., MDMA (Ecstasy) and the N-methylated form, methamphetamine. Amphetamine is a homologue of phenethylamine.
Traditionally the medical drug came in the racemic salt-form rac-amphetamine sulfate (rac = levo- and dextro-form in equal amounts). Today, dextroamphetamine sulphate is the predominant form of the drug used; it consists entirely of the d-isomer. Attention disorders are often treated using Adderall or generic-equivalent formulations of mixed amphetamine salts that contain both d/l-amphetamine and d-amphetamine in the sulfate and saccharate forms mixed to a final ratio of 3 parts d-amphetamine to 1 part l-amphetamine.
Pharmacology
Dextroamphetamine, the eutomer of amphetamine, exhibits its mode of peripheral action via release and reuptake inhibition of the monoamine neurotransmitters acetylcholine (ACh) and histamine (H), but not glutamate. Its activity at the vesicular monoamine transporter VMAT2 is of crucial importance in the release process.[1]
Application range
Amphetamine is a synthetic drug with strong stimulant effects. In the United States, it is most commonly used for treatment of attention-deficit disorders and narcolepsy, but is also approved as a weight-loss medication in certain cases of obesity. Within the armed forces only, it is also frequently prescribed as an anti-fatigue pill for pilots and other individuals in situations requiring vigilance and alertness. Amphetamine is also used illegally to take advantage of these effects. The wanted effects stem predominantly from d-amphetamine; l-amphetamine contributes to the unwanted peripheral side effects, primarily nausea after the dose loses effect.
Medicinal use
Indicated for:
Recreational uses: Other uses:
|
Contraindications:
|
Side effects:
Cardiovascular: Ear, nose, and throat: Eye:
Gastrointestinal:
Musculoskeletal:
Neurological:
Respiratory: |
The experimental medical use of amphetamines began in the 1920s. It was introduced in most of the world in the form of the pharmaceutical Benzedrine in the late-1920s. The drug was used by the militaries of several nations, especially the air forces, to fight fatigue and increase alertness among servicemen. After decades of reports of abuse, the FDA banned Benzedrine inhalers, and limited amphetamines to prescription use in 1959, but illegal use became common.
Along with methylphenidate (Ritalin, Concerta, etc.), amphetamine is one of the standard treatments for ADHD. Beneficial effects for ADHD can include improved impulse control, improved concentration, decreased sensory overstimulation, and decreased irritability. These effects can be dramatic, particularly in young children. The ADHD medication Adderall is composed of four different amphetamine salts, and Adderall XR is a timed release formulation of these same salt forms.
When used within the recommended doses, side-effects like loss of appetite tend to decrease over time. However, amphetamines last longer in the body than methylphenidate (Ritalin, Concerta, etc.), and tend to have stronger side-effects on appetite and sleep.
Amphetamines are also a standard treatment for narcolepsy as well as other sleeping disorders. They are generally effective over long periods of time without producing addiction or physical dependence.
Amphetamines are sometimes used to augment anti-depressant therapy in treatment-resistant depression.
Medical use for weight loss is still approved in some countries, but is regarded as obsolete and dangerous in, for example, the United States.
Effects of use
Amphetamines release stores of norepinephrine and dopamine from nerve endings by converting the respective molecular transporters into open channels. Amphetamine also releases stores of serotonin from synaptic vesicles. Like methylphenidate (Ritalin), amphetamines also prevent the monoamine transporters for dopamine and norepinephrine from recycling them (called reuptake inhibition), which leads to increased amounts of dopamine and norepinephrine in synaptic clefts.
These combined effects rapidly increase the concentrations of the respective neurotransmitters in the synaptic cleft, which promotes nerve impulse transmission in neurons that have those receptors.
Physical effects
- Short-term physiological effects include decreased appetite, increased stamina and physical energy, increased sexual drive/response, involuntary bodily movements, hyperhidrosis, hyperactivity, jitteriness, nausea, itchy, blotchy or greasy skin, Tachycardia, irregular heart rate, hypertension, and headaches. Fatigue can often follow the dose's period of effectiveness. Overdose can be treated with chlorpromazine. [1]
- Long-term abuse or overdose effects can include tremor, restlessness, changed sleep patterns, anxiety and increase in pre-existing anxiety, poor skin condition, hyperreflexia, tachypnea, gastrointestinal narrowing, and weakened immune system. Fatigue and depression can follow the excitement stage. Erectile dysfunction, heart problems, stroke, and liver, kidney and lung damage can result from prolonged use. When snorted, amphetamine can lead to a deterioration of the lining of the nostrils.
Psychological effects
- Short-term psychological effects can include alertness, euphoria, increased concentration, rapid talking, increased confidence, increased social responsiveness, nystagmus (eye wiggles), hallucinations, and loss of REM sleep the night after use.
- Long-term psychological effects can include insomnia, mental states resembling schizophrenia, aggressiveness (not associated with schizophrenia), addiction or dependence with accompanying withdrawal symptoms, irritability, confusion, and panic. Chronic and/or extensively-continuous use can lead to amphetamine psychosis, which causes delusions and paranoia, but this is uncommon when taken as prescribed. Amphetamine is highly-psychologically addictive, and, with chronic use, tolerance develops very quickly. Withdrawal is, although not physiologically threatening, an unpleasant experience (including paranoia, depression, difficult breathing, dysphoria, gastric fluctuations and/or pain, and lethargia). This commonly leads chronic users to re-dose amphetamine frequently, explaining tolerance and increasing the possibility of addiction.
Addiction
Tolerance is developed rapidly in amphetamine use, therefore increasing the amount of the drug that is needed to satisfy the addiction. Many abusers will repeat the amphetamine cycle by taking more of the drug during the withdrawal. This leads to a very dangerous cycle and may involve the use of other drugs to get over the withdrawal process. Chronic users of amphetamines may resort to drug injection to experience the full effect of the drug in a faster and more intense way, with the added risks of bacterial and viral tranmission, vein damage and higher risk of overdose.
Legal issues
- In the United Kingdom, amphetamines are regarded as Class B drugs. The maximum penalty for unauthorised possession is three months' imprisonment and a £2,500 fine.
- In the United States, amphetamine and methamphetamine are Schedule II controlled drugs, classified as a CNS (Central Nervous System) Stimulant. A Schedule II drug is classified as one that: has a high potential for abuse, has a currently-accepted medical use and is used under severe restrictions, and has a high possibility of severe psychological and physiological dependence.
Internationally, amphetamine is a Schedule II drug under the Convention on Psychotropic Substances[2].
Popular culture
- Avant-garde rock and roll band The Velvet
Underground wrote White Light/White Heat (song), about
the effects of the drug.
Blues-Rock band Canned Heat wrote a song, on the album Boogie With Canned Heat called Amphetamine Annie, about a girl who takes speed regularly.
Rock and roll band Everclear (band) wrote a song called Amphetamine, about a girl named Amphetamine.
Space-rock band Hawkwind performed a song entitled "Motorhead", written by Lemmy Kilmister shortly before forming his own band of the same name. Kilmister is known for being a longtime user of speed.
Alternative Rock band The Smashing Pumpkins mention Amphetamine in a song titled "Annie Dog" from the album "Adore".
Rock and Roll band The Sisters of Mercy were (in)famous for the constant references to amphetamine throughout their career.
Industrial Rock band Marilyn Manson mention Amphetamines in a song titled "Rock is Dead".
Punk rock band Toys That Kill have a song entitled Amphetamine St. off their album The Citizen Abortion.
Alternative Metal band Seether mention Amphetamine in a song titled "I'm The One" from the album "Karma And Effect".
Books
- Seabrook, Jeremy (1996). In the Cities of the South:scenes from a developing world. London; New York: Verso. ISBN 1-85984-986-5.
Related pages
- Adderall
- Methamphetamine (Desoxyn)
- Methylphenidate (Ritalin, Concerta)
- Phenethylamines
- Stimulants
External links
- CID 5826 from PubChem (D-form dextroamphetamine)
- CID 3007 from PubChem (L-form and D,L-forms)
- CID 32893 from PubChem (L-form Levamphetamine or L-amphetamine)
- Erowid - Amphetamines
- The Good Drugs Guide - Amphetamines
- Lycaeum - Amphetamines
- SpeedSmart.org: Support for Safe and Successful Stimulant Use
- Srisurapanont et al, Treatment for amphetamine dependence and abuse
- Drugs.com - Amphetamine
- Asia & Pacific Amphetamine-Type Simulants Information Centre
- - Information and harm reduction strategies for amphetamines and other illicit drugs
- Amphetamines news page - Alcohol and Drugs History Society
References and Notes
- ^ D. Sulzer (2005). "Mechanisms of neurotransmitter release by amphetamines: a review". Prog. Neurobiol. 75 (6): 406-33. PMID 15955613.
- ^ List of psychotropic substances under international control (PDF). International Narcotics Control Board. Retrieved on November 19, 2005.
