


 216.73.216.133
216.73.216.133 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 216.73.xxx.xxx
216.73.xxx.xxx
 Server Time:
Server Time:
 |
|
|
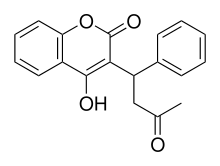
Warfarin
|
|
| Systematic (IUPAC) name | |
|
(RS)-4-hydroxy-3-(3-oxo-1-phenylbutyl)- 2H-chromen-2-one |
|
| Identifiers | |
| CAS number | 81-81-2 |
| ATC code | B01AA03 |
| PubChem | 6691 |
| DrugBank | APRD00341 |
| Chemical data | |
| Formula | C19H16O4 |
| Mol. weight | 308.33 g/mol |
| Pharmacokinetic data | |
| Bioavailability | 100% |
| Protein binding | 99.5% |
| Metabolism | Hepatic: CYP2C9, 2C19, 2C8, 2C18, 1A2 and 3A4 |
| Half life | 2.5 days |
| Excretion | Renal (92%) |
| Therapeutic considerations | |
| Pregnancy cat. | D(AU) X(US) |
| Legal status | S4(AU) POM(UK) ℞-only(US) |
| Routes | Oral |
Warfarin (also known under the brand names of Coumadin®, Jantoven®, Marevan®, and Waran®) is an anticoagulant medication that is administered orally or, very rarely, by injection. It is used for the prophylaxis of thrombosis and embolism in many disorders. Its activity has to be monitored by frequent blood testing for the international normalized ratio (INR). It is named for the Wisconsin Alumni Research Foundation.
Warfarin is a synthetic derivative of coumarin, a chemical found naturally in many plants, notably woodruff (Galium odoratum, Rubiaceae), and at lower levels in licorice, lavender and various other species. Warfarin was originally developed as a rat poison, but it is no longer used for that purpose as modern poisons are much more potent and toxic (e.g. brodifacoum). However, warfarin and contemporary rodenticides belong to the same class of drugs (coumarins) and both decrease blood coagulation by interfering with vitamin K metabolism.
Contents |
Mechanism of action
Warfarin inhibits the synthesis of biologically active forms of the vitamin K-dependent clotting factors: II, VII, IX and X, as well as the regulatory factors protein C, protein S and protein Z. Other proteins not involved in blood clotting, such as osteocalcin, or matrix Gla protein, may also be affected.
The precursors of these factors require carboxylation of their glutamic acid residues to allow the coagulation factors to bind to phospholipid surfaces inside blood vessels, on the vascular endothelium. This enzyme that carries out the carboxylation of glutamic acid is the gamma-glutamyl carboxylase. The carboxylation reaction will only proceed if the carboxylase enzyme is able to convert a reduced form of Vitamin K (Vitamin K hydroquinone) to vitamin K epoxide at the same time. The Vitamin K epoxide is in turn recycled back to Vitamin K and Vitamin K hydroquinone by another enzyme, the vitamin K epoxide reductase (VKOR). Warfarin inhibits epoxide reductase[1] (specifically the VKORC1 subunit[2][3]), thereby diminishing available vitamin K and Vitamin K hydroqunone in the tissues, which inhibits the carboxylation activity of the glutamyl carboxylase. When this occurs, the coagulation factors are no longer carboxylated at certain glutamic acid residues, and are incapable of binding to the endothelial surface of blood vessels, and are thus biologically inactive. As the body stores of previously-produced active factors degrade (over several days) and are replaced by inactive factors, the anticoagulation effect becomes apparent. The coagulation factors are produced, but have decreased functionality due to undercarboxylation; they are collectively referred to as PIVKAs (proteins induced [by] vitamin K absence/antagonism). Hence, the effect of warfarin is to diminish blood clotting in the patient.
Uses
Medical use
Warfarin is prescribed to people with an increased tendency for thrombosis or as prophylaxis in those individuals who have already formed a blood clot (thrombus) which required treatment. This can help prevent formation of future blood clots and help reduce the risk of embolism (migration of a thrombus to a spot where it blocks blood supply to a vital organ). Common clinical indications for warfarin use are atrial fibrillation, artificial heart valves, deep venous thrombosis and pulmonary embolism.[4]
Dosing of warfarin is complicated by the fact that it is known to interact with many commonly used medications and other chemicals that may be present in appreciable quantities in food. These interactions may enhance or reduce warfarin's anticoagulation effect. Many commonly used antibiotics, such as metronidazole or the macrolides, will greatly increase the effect of warfarin by reducing the metabolism of warfarin in the body. Other broad-spectrum antibiotics can reduce the amount of the normal bacterial flora in the bowel, which make significant quantities of Vitamin K, thus potentiating the effect of warfarin. In addition, food that contains large quantities of Vitamin K will reduce the warfarin effect; and medical conditions such as hypo- or hyperthyroidism will alter the rate of breakdown of the clotting factors.
Therefore, in order to optimise the therapeutic effect without risking dangerous side effects, such as bleeding, close monitoring of the degree of anticoagulation is required by blood testing (INR). Initially, checking may be as often as twice a week; the intervals can be lengthened if the patient manages stable therapeutic INR levels on an unchanged warfarin dose.
When initiating warfarin therapy ("warfarinisation"), the doctor will decide how strong the anticoagulant therapy needs to be. The target INR level will vary from case to case dependent upon the clinical indicators, but tends to be 2-3 in most conditions.
The oral anticoagulant ximelagatran (Exanta®) was expected to replace warfarin to a large degree when introduced; however, reports of hepatotoxicity (liver damage) prompted its manufacturer to withdraw it from further development. Other drugs offering the efficacy of warfarin without a need for monitoring, such as dabigatran and rivaroxaban, are under development.
Pesticide use
Coumarins, a class of drugs of which warfarin is a member, are used as a rodenticide for controlling rats and mice in residential, industrial, and agricultural areas. The active ingredient in rat poison is brodifacoum, which is sometimes referred to as a super-warfarin, because it is longer acting than the drug warfarin. It is both odorless and tasteless. It is effective when mixed with food bait, because the rodents will return to the bait and continue to feed over a period of days, until a lethal dose is accumulated (considered to be 1 mg/kg b.w./day over four to five days for warfarin; for brodifacoum, no reliable cumulative toxicity datas are available as of time, but it could be concluded, given the similarity with other 4-hydroxycoumarin derivatives, that these would be in order of tens of µg/kg b.w./day for periods of 2-10 days). It may also be mixed with talc and used as a tracking powder, which accumulates on the animal's skin and fur, and is subsequently consumed during grooming. The use as rat poison is now declining because many rat populations have developed resistance to warfarin.
The LD50 is 50500 mg/kg. The IDLH value is 100mg/m³ (warfarin; various species). LD50(mouse, oral) = 0.40 mg/kg; (rat, oral) = 0.27 mg/kg (brodifacoum). The IDLH value for brodifacoum is not defined, but given the toxicity of brodifacoum, it would be substantialy lower, perhaps less than 1/100 of the warfarin value, i.e. <1 mg/m³.
Side-effects
The only common side-effect of warfarin is hemorrhage (bleeding). The risk of severe bleeding is small but definite (1-2% annually) and any benefit needs to outweigh this risk when warfarin is considered as a therapeutic measure. Risk of bleeding is augmented if the INR is out of range (due to accidental or deliberate overdose or due to interactions), and may cause hemoptysis (coughing up blood), excessive bruising, bleeding from nose or gums, or blood in urine or stool.
A feared (but rare) complication of warfarin is warfarin necrosis, which occurs more frequently shortly after commencing treatment in patients with a deficiency of protein C. Protein C is an innate anticoagulant that, like the procoagulant factors that warfarin inhibits, requires vitamin K-dependent carboxylation for its activity. Since warfarin initially decreases protein C levels faster than the coagulation factors, it can paradoxically increase the blood's tendency to coagulate when treatment is first begun (many patients when starting on warfarin are given heparin in parallel to combat this), leading to massive thrombosis with skin necrosis and gangrene of limbs. Its natural counterpart, purpura fulminans, occurs in children who are homozygous for protein C mutations.
Pharmacology

Pharmacokinetics and antagonism
Warfarin consists of a racemic mixture of two active optical isomers - R and S forms - each of which is cleared by different pathways. S-warfarin has five times the potency of the R-isomer with respect to Vitamin K antagonism.[4]
Warfarin is slower acting than the common anticoagulant heparin, though it has a number of advantages. Heparin must be given by injection, while warfarin is available orally. Warfarin has a long half-life and need only be given once a day. Heparin can also cause a prothrombotic condition, heparin-induced thrombocytopenia (an antibody-mediated decrease in platelet levels), which paradoxically increases the risk for thrombosis. Warfarin's long half life, on the other hand, means it often takes several days to reach therapeutic effect. Furthermore, if given initially without additional anticoagulant cover, it can paradoxically increase thrombosis risk. For these main reasons, hospitalised patients are usually given heparin initially, and are then moved on to warfarin.
Warfarin can be reversed with vitamin K, or for rapid reversal (e.g. in case of severe bleeding), with fresh frozen plasma but this treatment is being replaced by use of prothrombin complex concentrate.
Pharmacogenomics
Warfarin activity is determined partially by genetic factors. Polymorphisms in the VKORC1 gene explain 25% of the dose variation between patients: particular mutations make VKORC1 less susceptible to suppression by warfarin.[3][5] CYP2C9 polymorphisms explain another 10%.[5] VKORC1 polymorphisms also explain why African Americans are relatively resistant to warfarin, while Asian Americans are more sensitive.[5] Small Text
Loading regimens
Because of warfarin's poorly predictable pharmacokinetics, several researchers have proposed algorithms for commencing warfarin treatment. For urgent anticoagulation, the Fennerty regimen[6] is used commonly, while for "routine" (low-risk) anticoagulation, the Tait regimen[7] is more popular.
Interactions and contraindications
There are many drug-drug interactions with warfarin, and its metabolism varies greatly between patients. Some foodstuffs have also been reported to interact with warfarin[8] This makes finding the correct dosage difficult, and accentuates the need of monitoring; when initiating a medication that is known to interact with warfarin (e.g. amiodarone), INR checks are increased or dosages adjusted until a new ideal dosage is found.
Warfarin cannot be given to pregnant women, especially in the first trimester, as it is a teratogen (it causes deformations of the face and bones). During the third trimester, antepartum hemorrhage can occur. Instead of warfarin, low molecular weight heparin is generally used.
Excessive use of alcohol is also known to affect the metabolism of warfarin, although moderate drinking usually has little or no effect on the INR value. Patients suffering from liver damage or alcoholism are usually treated with heparin injections instead.
Warfarin also interacts with the following herbs: [9]
- Ginkgo (a.k.a. Ginkgo Biloba), which is commonly used to increase brain blood flow, prevent dementia, and improve memory. However, ginkgo may increase blood pressure, and may increase bleeding, especially in people already taking certain anti-clotting medications such as warfarin.
- St. John's Wort is commonly used to help with mild to moderate depression. However, it may prolong the effects of certain anesthetic drugs and reduce the effects oral contraceptives and anti-organ transplant rejection medications, and interfere with warfarin.
- Ginseng is commonly used to help with fatigue and weakness. However, ginseng may increase blood pressure and heart rate and may increase bleeding, especially in people already taking certain anti-clotting medications such as warfarin.
- Garlic (as a supplement, not in the diet) is commonly used to help lower high cholesterol levels, high triglycerides, and high blood pressure. However, may increase bleeding especially in people already taking certain anti-clotting medications such as warfarin.
- Ginger is commonly used to help nausea and poor digestion. However, it may increase bleeding, especially in patients already taking certain anti-clotting medications such as warfarin.
History
The early 1920s saw the outbreak of a previously unrecognized disease of cattle in the northern United States and Canada. Cattle would die of uncontrollable bleeding from very minor injuries, or sometimes drop dead of internal hemorrhage with no external signs of injury. In 1921, Frank Schofield, a Canadian veterinarian, determined that the cattle were ingesting moldy silage made from sweet clover that functioned as a potent anticoagulant.[10] In 1929, North Dakota veterinarian Dr L.M. Roderick demonstrated that the condition was due to a lack of functioning prothrombin.[11]
The identity of the anticoagulant substance in moldy sweet clover remained a mystery until 1940 when Karl Paul Link and his student Harold Campbell, chemists working at the University of Wisconsin, determined that it was the coumarin derivative 4-hydroxycoumarin.[12] Over the next few years, numerous similar chemicals were found to have the same anticoagulant properties. The first of these to be widely commericialized was dicoumarol, patented in 1941. Link continued working on developing more potent coumarin-based anticoagulants for use as rodent poisons, resulting in warfarin in 1948. (The name warfarin stems from the acronym WARF, for Wisconsin Alumni Research Foundation + the ending -arin indicating its link with coumarin. Warfarin was first registered for use as a rodenticide in the US in 1952; although it was developed by Link, the WARF financially supported the research and was granted the patent.
The exact mechanism of action remained unknown until it was demonstrated, in 1978, that warfarin inhibited epoxide reductase and hence interfered with vitamin K metabolism.[1]
After an incident in 1951, where a naval enlisted man unsuccessfully attempted suicide with warfarin and recovered fully, studies began in the use of warfarin as a therapeutic anticoagulant. It was found to be generally superior to dicoumarol, and in 1954 was approved for medical use in humans. A famous early patient prescribed warfarin was Dwight Eisenhower, president of the USA, subsequent to his heart attack in 1955.
A 2003 theory posits that warfarin was used by a conspiracy of Lavrenty Beria, Nikita Khrushchev and others to poison Soviet leader Joseph Stalin. Warfarin is tasteless and colorless, and produces symptoms similar to those that Stalin exhibited.[13]
Other coumarins
In some countries, other coumarins are used instead of warfarin, such as acenocoumarol and phenprocoumon. These have a shorter (acenocoumarol) or longer (phenprocoumon) half-life, and are not completely interchangeable with warfarin.
References
- ^ a b Whitlon DS, Sadowski JA, Suttie JW. Mechanisms of coumarin action: significance of vitamin K epoxide reductase inhibition. Biochemistry 1978;17:13717. PMID 646989.
- ^ Li T, Chang CY, Jin DY, Lin PJ, Khvorova A, Stafford DW. Identification of the gene for vitamin K epoxide reductase. Nature 2004;427(6974):541-4. PMID 14765195.
- ^ a b Rost S, Fregin A, Ivaskevicius V, Conzelmann E, Hortnagel K, Pelz HJ, Lappegard K, Seifried E, Scharrer I, Tuddenham EG, Muller CR, Strom TM, Oldenburg J. Mutations in VKORC1 cause warfarin resistance and multiple coagulation factor deficiency type 2. Nature 2004;427(6974):537-41. PMID 14765194.
- ^ a b Hirsh J, Fuster V, Ansell J, Halperin JL. American Heart Association/American College of Cardiology Foundation guide to Warfarin therapy. J Am Coll Cardiol 2003;41:1633-52. PMID 12742309.
- ^ a b c Rieder MJ, Reiner AP, Gage BF, Nickerson DA, Eby CS, McLeod HL, Blough DK, Thummel KE, Veenstra DL, Rettie AE. Effect of VKORC1 haplotypes on transcriptional regulation and warfarin dose. N Engl J Med 2005;352:2285-93. PMID 15930419.
- ^ Fennerty A, Campbell IA, Routledge PA. Anticoagulants in venous thromboembolism. BMJ 1988;297:1285-8. PMID 3144365.
- ^ Tait RC, Sefcick A. A warfarin induction regimen for out-patient anticoagulation in patients with atrial fibrillation. Br J Haematol 1998;101:450-4. PMID 9633885.
- ^ Holbrook AM, Pereira JA, Labiris R, McDonald H, Douketis JD, Crowther M, Wells PS. Systematic overview of warfarin and its drug and food interactions. Arch Intern Med 2005;165:1095-106. PMID 15911722.
- ^ Austin, Steve, and Forrest Batz. The A-Z Guide to Drug-Herb-Vitamin Interactions: How to Improve Your Health and Avoid Problems When Using Common Medications and Natural Supplements Together. Ed. Schulyer M. Lininger. 1st ed. New York: Three Rivers P, 1999. p.224.
- ^ Schofield FW. Damaged sweet clover; the cause of a new disease in cattle simulating haemorrhagic septicemia and blackleg. J Am Vet Med Ass 1924;64:553-6.
- ^ Roderick LM. A problem in the coagulation of the blood; "sweet clover disease of the cattle". Am J Physiol 1931;96:413-6.
- ^ Stahmann MA, Huebner CF, Link KP. Studies on the hemorrhagic sweet clover disease. V. Identification and synthesis of the hemorrhagic agent. J Biol Chem 1941;138:513-27 PDF.
- ^ Jonathan Brent, Vladimir Naumov. Stalin's Last Crime : The Plot Against the Jewish Doctors, 1948-1953. HarperCollins, 2003. ISBN 0-06-019524-X.
External links
- Warfarin pesticide profile from US Department of Agriculture
- Warfarin
- Historical information on Warfarin
- Warfarin factsheet from the Royal Society of Chemistry
