


 216.73.216.16
216.73.216.16 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 216.73.xxx.xx
216.73.xxx.xx
 Server Time:
Server Time:
 |
||
|---|---|---|
| Young asthmatic girl using an inhaler attached to a spacer. | ||
| ICD-10 | J45. | |
| ICD-9 | 493 | |
| OMIM | 600807 | |
| DiseasesDB | 1006 | |
| MedlinePlus | 000141 | |
| eMedicine | med/177 emerg/43 | |
| MeSH | C08.127.108 | |
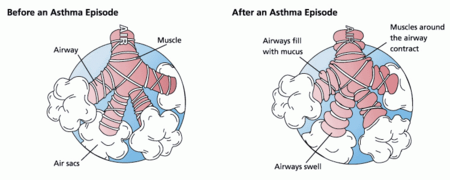
Asthma is a disease of the respiratory system in which the airways constrict, become inflamed, and are lined with excessive amounts of mucus, often in response to one or more "triggers," such as exposure to an environmental stimulant (or allergen), cold air, exercise, or emotional stress. In children, the most common triggers are viral illnesses such as those that cause the common cold.[1] This airway narrowing causes symptoms such as wheezing, shortness of breath, chest tightness, and coughing, which respond to bronchodilators. Between episodes, most patients feel fine.
The disorder is a chronic or recurring inflammatory condition in which the airways develop increased responsiveness to various stimuli, characterized by bronchial hyper-responsiveness, inflammation, increased mucus production, and intermittent airway obstruction. The symptoms of asthma, which can range from mild to life threatening, can usually be controlled with a combination of drugs and enviromental changes.
Public attention in the developed world has recently focused on asthma because of its rapidly increasing prevalence, affecting up to one in four urban children.[2] Susceptibility to asthma can be explained in part by genetic factors, but no clear pattern of inheritance has been found. Asthma is a complex disease that is influenced by multiple genetic, developmental, and environmental factors, which interact to produce the overall condition.
Contents |
History
The word asthma is derived from the Greek aazein, meaning "sharp breath." The word first appears in Homer's Iliad;[3] Hippocrates was the first to use it in reference to the medical condition. Hippocrates thought that the spasms associated with asthma were more likely to occur in tailors, anglers, and metalworkers. Six centuries later, Galen wrote much about asthma, noting that it was caused by partial or complete bronchial obstruction. Moses Maimonides, an influential medieval rabbi, philosopher, and physician, wrote a treatise on asthma, describing its prevention, diagnosis, and treatment.[4] In the 17th century, Bernardino Ramazzini noted a connection between asthma and organic dust. The use of bronchodilators started in 1901, but it was not until the 1960s that the inflammatory component of asthma was recognized, and anti-inflammatory medications were added to the regimen.
Signs and symptoms
In some individuals asthma is characterized by chronic respiratory impairment. In others it is an intermittent illness marked by episodic symptoms that may result from a number of triggering events, including upper respiratory infection, airborne allergens, and exercise.
An acute exacerbation of asthma is referred to as an asthma attack. The clinical hallmarks of an attack are shortness of breath (dyspnea) and either wheezing or stridor. Although the latter is "often regarded as the sine qua non of asthma,"[5] some victims present primarily with coughing, and in the late stages of an attack, air motion may be so impaired that no wheezing may be heard. When present the cough may sometimes produce clear sputum. The onset may be sudden, with a sense of constriction in the chest, breathing becomes difficult, and wheezing occurs (primarily upon expiration, but can be in both respiratory phases).
Signs of an asthmatic episode or asthma attack are either stridor or wheezing, rapid breathing (tachypnea), prolonged expiration, a rapid heart rate (tachycardia), rhonchous lung sounds (audible through a stethoscope), and over-inflation of the chest. During a serious asthma attack, the accessory muscles of respiration (sternocleidomastoid and scalene muscles of the neck) may be used, shown as in-drawing of tissues between the ribs and above the sternum and clavicles, and the presence of a paradoxical pulse (a pulse that is weaker during inhalation and stronger during exhalation).
During very severe attacks, an asthma sufferer can turn blue from lack of oxygen, and can experience chest pain or even loss of consciousness. Severe asthma attacks may lead to respiratory arrest and death. Despite the severity of symptoms during an asthmatic episode, between attacks an asthmatic may show few signs of the disease.
Diagnosis
In most cases, a physician can diagnose asthma on the basis of typical findings in a patient's clinical history and examination. Asthma is strongly suspected if a patient suffers from eczema or other allergic conditionssuggesting a general atopic constitutionor has a family history of asthma. While measurement of airway function is possible for adults, most new cases are diagnosed in children who are unable to perform such tests. Diagnosis in children is based on a careful compilation and analysis of the patient's medical history and subsequent improvement with an inhaled bronchodilator medication. In adults, diagnosis can be made with a peak flow meter (which tests airway restriction), looking at both the diurnal variation and any reversibility following inhaled bronchodilator medication.
Testing peak flow at rest (or baseline) and after exercise can be helpful, especially in young asthmatics who may experience only exercise-induced asthma. If the diagnosis is in doubt, a more formal lung function test may be conducted. Once a diagnosis of asthma is made, a patient can use peak flow meter testing to monitor the severity of the disease.
Differential diagnosis
Before diagnosing someone as asthmatic, alternative possibilities should be considered. A physician taking a history should check whether the patient is using any known bronchoconstrictors (substances that cause narrowing of the airways, e.g., certain anti-inflammatory agents or beta-blockers).
Chronic obstructive pulmonary disease, which closely resembles asthma, is correlated with more exposure to cigarette smoke, an older patient, less symptom reversibility after bronchodilator administration (as measured by spirometry), and decreased likelihood of family history of atopy.
Pulmonary aspiration, whether direct due to dysphagia (swallowing disorder) or indirect (due to acid reflux), can show similar symptoms to asthma. However, with aspiration, fevers might also indicate aspiration pneumonia. Direct aspiration (dysphagia) can be diagnosed by performing a Modified Barium Swallow test and treated with feeding therapy by a qualified speech therapist. If the aspiration is indirect (from acid reflux) then treatment directed at this is indicated.
Only a minority of asthma sufferers have an identifiable allergy trigger. The majority of these triggers can often be identified from the history; for instance, asthmatics with hay fever or pollen allergy will have seasonal symptoms, those with allergies to pets may experience an abatement of symptoms when away from home, and those with occupational asthma may improve during leave from work. Occasionally, allergy tests are warranted and, if positive, may help in identifying avoidable symptom triggers.
After pulmonary function has been measured, radiological tests, such as a chest X-ray or CT scan, may be required to exclude the possibility of other lung diseases. In some people, asthma may be triggered by gastroesophageal reflux disease, which can be treated with suitable antacids. Very occasionally, specialized tests after inhalation of methacholine or, even less commonly, histamine may be performed.
Asthma is categorized by the United States National Heart, Lung and Blood Institute as falling into one of four categories: mild intermittent, mild persistent, moderate persistent and severe persistent. The diagnosis of "severe persistent asthma" occurs when symptoms are continual with frequent exacerbations and frequent nighttime symptoms, result in limited physical activity and when lung function as measured by PEV or FEV1 tests is less than 60% predicted with PEF variability greater than 30%.
There is no cure for asthma. Doctors have only found ways to prevent attacks and relieve the symptoms such as tightness of the chest and trouble breathing.
Pathophysiology
Bronchoconstriction
In essence, asthma is the result of an immune response in the bronchial airways.[6]
The airways of asthmatics are "hypersensitive" to certain triggers, also known as stimuli (see below). In response to exposure to these triggers, the bronchi (large airways) contract into spasm (an "asthma attack"). Inflammation soon follows, leading to a further narrowing of the airways and excessive mucus production, which leads to coughing and other breathing difficulties.
There are several categories of stimuli:
- allergenic air pollution, from nature, typically inhaled, which include waste from common household insects, such as the house dust mite and cockroach, grass pollen, mould spores and pet epithelial cells;
- medications, including aspirin[7] and β-adrenergic antagonists (beta blockers);
- Use of fossil fuel related allergenic air pollution, such as ozone, Smog, Summer smog, nitrogen dioxide, and sulfur dioxide, which is thought to be one of the major reasons for the high prevalence of asthma in urban areas;
- various industrial compounds and other chemicals, notably sulfites; chlorinated swimming pools generate chloraminesmonochloramine (NH2Cl), dichloramine (NHCl2) and trichloramine (NCl3)in the air around them, which are known to induce asthma.[8]
- early childhood infections, especially viral respiratory infections. However, persons of any age can have asthma triggered by colds and other respiratory infections even though their normal stimuli might be from another category (e.g. pollen) and absent at the time of infection. 80% of asthma attacks in adults and 60% in children are caused by respiratory viruses.
- exercise, the effects of which differ somewhat from those of the other triggers;
- (in some countries) - allergenic indoor air pollution from Newsprint & other literature such as, junk mail leaflets & glossy magazines.
- emotional stress which is poorly understood as a trigger. Perhaps because crying might be a form of exercise or because being given an asthma attack may be distressing.
Bronchial inflammation
The mechanisms behind allergic asthmai.e., asthma resulting from an immune response to inhaled allergensare the best understood of the causal factors. In both asthmatics and non-asthmatics, inhaled allergens that find their way to the inner airways are ingested by a type of cell known as antigen presenting cells, or APCs. APCs then "present" pieces of the allergen to other immune system cells. In most people, these other immune cells (TH0 cells) "check" and usually ignore the allergen molecules. In asthmatics, however, these cells transform into a different type of cell (TH2), for reasons that are not well understood. The resultant TH2 cells activate an important arm of the immune system, known as the humoral immune system. The humoral immune system produces antibodies against the inhaled allergen. Later, when an asthmatic inhales the same allergen, these antibodies "recognize" it and activate a humoral response. Inflammation results: chemicals are produced that cause the airways to constrict and release more mucus, and the cell-mediated arm of the immune system is activated. The inflammatory response is responsible for the clinical manifestations of an asthma attack. The following section describes this complex series of events in more detail.
Pathogenesis
The fundamental problem in asthma appears to be immunological: young children in the early stages of asthma show signs of excessive inflammation in their airways. Epidemiological findings give clues as to the pathogenesis: the incidence of asthma seems to be increasing worldwide, and asthma is now very much more common in affluent countries.
In 1968 Andor Szentivanyi first described The Beta Adrenergic Theory of Asthma; in which blockage of the Beta-2 receptors of pulmonary smooth muscle cells causes asthma.[9] Szentivanyi's Beta Adrenergic Theory is a citation classic[10] and has been cited more times than any other article in the history of the Journal of Allergy.
In 1995 Szentivanyi and colleagues demonstrated that IgE blocks beta-2 receptors.[11] Since overproduction of IgE is central to all atopic diseases, this was a watershed moment in the world of Allergy.[12]
The Beta-Adrenergic Theory has been cited in the scholarship of such noted investigators as Richard F. Lockey (former President of The American Academy of Allergy, Asthma, and Immunology),[13] Charles Reed (Chief of Allergy at Mayo Medical School),[14] and Craig Venter (Human Genome Project).[15]
One theory of pathogenesis is that asthma is a disease of hygiene. In nature, babies are exposed to bacteria and other antigens soon after birth, "switching on" the TH1 lymphocyte cells of the immune system that deal with bacterial infection. If this stimulus is insufficientas it may be in modern, clean environmentsthen TH2 cells predominate, and asthma and other allergic diseases may develop. This "hygiene hypothesis" may explain the increase in asthma in affluent populations. The TH2 lymphocytes and eosinophil cells that protect us against parasites and other infectious agents are the same cells responsible for the allergic reaction. The Charcot-Leyden crystals are formed when the crystalline material in eosinophils coalesce. These crystals are significant in sputum samples of people with asthma. In the developed world, these parasites are now rarely encountered, but the immune response remains and is wrongly triggered in some individuals by certain allergens.
Another theory is based on the correlation of air pollution and the incidence of asthma. Although it is well known that substantial exposures to certain industrial chemicals can cause acute asthmatic episodes, it has not been proven that air pollution is responsible for the development of asthma. In Western Europe, most atmospheric pollutants have fallen significantly over the last 40 years, while the prevalence of asthma has risen.
Finally, it has been postulated that some forms of asthma may be related to infection, in particular by Chlamydia pneumoniae.[16] This issue remains controversial, as the relationship is not borne out by meta-analysis of the research.[17] The correlation seems to be not with the onset, but rather with accelerated loss of lung function in adults with new onset of non-atopic asthma.[18] One possible explanation is that some asthmatics may have altered immune response that facilitates long-term chlamydia pneumonia infection.[19] The response to targeting with macrolide antibiotics has been investigated, but the temporary benefit reported in some studies may reflect just their anti-inflammatory activities rather than their antimicrobic action.[17]
Asthma and sleep apnea
It is recognized with increasing frequency, that patients who have both obstructive sleep apnea (OSA) and bronchial asthma, often improve tremendously when the sleep apnea is diagnosed and treated.[20] CPAP is not effective in patients with nocturnal asthma only.[21]
Asthma and gastro-esophageal reflux disease
If gastro-esophageal reflux disease is present, the patient may have repetitive episodes of acid aspiration, which results in airway inflammation and "irritant-induced" asthma. GERD may be common in difficult-to-control asthma, but generally speaking, treating it does not seem to affect the asthma.[22]
Treatment
The most effective treatment for asthma is identifying triggers, such as pets or aspirin, and limiting or eliminating exposure to them. Desensitization to allergens has been shown to be a treatment option for certain patients.[23]
As is common with respiratory disease, smoking adversely affects asthmatics in several ways, including an increased severity of symptoms, a more rapid decline of lung function, and decreased response to preventive medications.[24] Asthmatics who smoke typically require additional medications to help control their disease. Furthermore, exposure of both nonsmokers and smokers to secondhand smoke is detrimental, resulting in more severe asthma, more emergency room visits, and more asthma-related hospital admissions.[25] Smoking cessation and avoidance of secondhand smoke is strongly encouraged in asthmatics.[26]
The specific medical treatment recommended to patients with asthma depends on the severity of their illness and the frequency of their symptoms. Specific treatments for asthma are broadly classified as relievers, preventers and emergency treatment. The Expert panel report 2: Guidelines for the diagnosis and management of asthma (EPR-2)[26] of the U.S. National Asthma Education and Prevention Program, and the British guideline on the management of asthma[27] are broadly used and supported by many doctors. Bronchodilators are recommended for short-term relief in all patients. For those who experience occasional attacks, no other medication is needed. For those with mild persistent disease (more than two attacks a week), low-dose inhaled glucocorticoids or alternatively, an oral leukotriene modifier, a mast-cell stabilizer, or theophylline may be administered. For those who suffer daily attacks, a higher dose of glucocorticoid in conjunction with a long-acting inhaled β-2 agonist may be prescribed; alternatively, a leukotriene modifier or theophylline may substitute for the β-2 agonist. In severe asthmatics, oral glucocorticoids may be added to these treatments during severe attacks.
For those in whom exercise can trigger an asthma attack (exercise-induced asthma), higher levels of ventilation and cold, dry air tend to exacerbate attacks. For this reason, activities in which a patient breathes large amounts of cold air, such as skiing and running, tend to be worse for asthmatics, whereas swimming in an indoor, heated pool, with warm, humid air, is less likely to provoke a response.[5]
Researchers at Harvard Medical School (HMS) have come up with convincing evidence that the answer to what causes asthma lies in a special type of natural "killer" cell. This finding means that physicians may not be treating asthma sufferers with the right kinds of drugs. For example, natural killer T cells seem to be resistant to the corticosteroids in widely used inhalers.[28]
Relief medication
Symptomatic control of episodes of wheezing and shortness of breath is generally achieved with fast-acting bronchodilators. These are typically provided in pocket-sized, metered-dose inhalers (MDIs). In young sufferers, who may have difficulty with the coordination necessary to use inhalers, or those with a poor ability to hold their breath for 10 seconds after inhaler use (generally the elderly), an asthma spacer (see top image) is used. The spacer is a plastic cylinder that mixes the medication with air in a simple tube, making it easier for patients to receive a full dose of the drug and allows for the active agent to be dispersed into smaller, more fully inhaled bits. A nebulizerwhich provides a larger, continuous dosecan also be used. Nebulizers work by vaporizing a dose of medication in a saline solution into a steady stream of foggy vapour, which the patient inhales continuously until the full dosage is administered. There is no clear evidence, however, that they are more effective than inhalers used with a spacer. Nebulizers may be helpful to some patients experiencing a severe attack. Such patients may not be able to inhale deeply, so regular inhalers may not deliver medication deeply into the lungs, even on repeated attempts. Since a nebulizer delivers the medication continuously, it is thought that the first few inhalations may relax the airways enough to allow the following inhalations to draw in more medication.
Relievers include:
- Short-acting, selective beta2-adrenoceptor agonists, such as salbutamol (albuterol USAN), levalbuterol, terbutaline and bitolterol. Tremors, the major side effect, have been greatly reduced by inhaled delivery, which allows the drug to target the lungs specifically; oral and injected medications are delivered throughout the body. There may also be cardiac side effects at higher doses (due to Beta-1 agonist activity), such as elevated heart rate or blood pressure; with the advent of selective agents, these side effects have become less common. Patients must be cautioned against using these medicines too frequently, as with such use their efficacy may decline, producing desensitization resulting in an exacerbation of symptoms which may lead to refractory asthma and death.
- Older, less selective adrenergic agonists, such as inhaled epinephrine and ephedrine tablets, are available over the counter in the US. Cardiac side effects occur with these agents at either similar or lesser rates to albuterol.[29] [30] When used solely as a relief medication, inhaled epinephrine has been shown to be an effective agent to terminate an acute asthmatic exacerbation.[29] In emergencies, these drugs were sometimes administered by injection. Their use via injection has declined due to related adverse effects.
- Anticholinergic medications, such as ipratropium bromide may be used instead. They have no cardiac side effects and thus can be used in patients with heart disease; however, they take up to an hour to achieve their full effect and are not as powerful as the β2-adrenoreceptor agonists.
Prevention medication
Current treatment protocols recommend prevention medications such as an inhaled corticosteroid, which helps to suppress inflammation and reduces the swelling of the lining of the airways, in anyone who has frequent (greater than twice a week) need of relievers or who has severe symptoms. If symptoms persist, additional preventive drugs are added until the asthma is controlled. With the proper use of prevention drugs, asthmatics can avoid the complications that result from overuse of relief medications.
Asthmatics sometimes stop taking their preventive medication when they feel fine and have no problems breathing. This often results in further attacks, and no long-term improvement.
Preventive agents include the following.
- Inhaled glucocorticoids (ciclesonide, fluticasone, budesonide, beclomethasone, mometasone, flunisolide, and triamcinolone).
- Leukotriene modifiers (montelukast, zafirlukast, pranlukast, and zileuton).
- Mast cell stabilizers (cromoglicate (cromolyn), and nedocromil).
- Antimuscarinics/anticholinergics (ipratropium, oxitropium, and tiotropium), which have a mixed reliever and preventer effect. (These are rarely used in preventive treatment of asthma, except in patients who do not tolerate beta-2-agonists.)
- Methylxanthines (theophylline and aminophylline), which are sometimes considered if sufficient control cannot be achieved with inhaled glucocorticoids and long-acting β-agonists alone.
- Antihistamines, often used to treat allergic symptoms that may underlie the chronic inflammation. In more severe cases, hyposensitization ("allergy shots") may be recommended.
- Omalizumab, an IgE blocker; this can help patients with severe allergic asthma that does not respond to other drugs. However, it is expensive and must be injected.
- Methotrexate is occasionally used in some difficult-to-treat patients.
- If chronic acid indigestion (GERD) contributes to a patient's asthma, it should also be treated, because it may prolong the respiratory problem.
Long-acting β2-agonists

Long-acting bronchodilators (LABD) give a 12-hour effect, and are used to give a smoothed symptomatic effect (used morning and night). While patients report improved symptom control, these drugs do not replace the need for routine preventers, and their slow onset means the short-acting dilators may still be required. In November of 2005, the American FDA released a health advisory alerting the public to findings that show the use of Long-acting β2-agonists could lead to a worsening of symptoms, and in some cases death.[31]
Currently available long-acting beta2-adrenoceptor agonists include salmeterol, formoterol, bambuterol, and sustained-release oral albuterol. Combinations of inhaled steroids and long-acting bronchodilators are becoming more widespread; the most common combination currently in use is fluticasone/salmeterol (Advair in the United States, and Seretide in the UK).
A recent meta-analysis of the roles of long-acting beta-agonists may indicate a danger to asthma patients. "These agents can improve symptoms through bronchodilation at the same time as increasing underlying inflammation and bronchial hyper-responsiveness, thus worsening asthma control without any warning of increased symptoms," said Shelley Salpeter in a Cornel study. The study goes on to say that "Three common asthma inhalers containing the drugs salmeterol or formoterol may be causing four out of five U.S. asthma-related deaths per year and should be taken off the market".[32]
Emergency treatment
When an asthma attack is unresponsive to a patient's usual medication, other treatments are available to the physician or hospital:[33]
- oxygen to alleviate the hypoxia (but not the asthma per se) that results from extreme asthma attacks;
- nebulized salbutamol or terbutaline (short-acting beta-2-agonists), often combined with ipratropium (an anticholinergic);
- systemic steroids, oral or intravenous (prednisone, prednisolone, methylprednisolone, dexamethasone, or hydrocortisone)
- other bronchodilators that are occasionally
effective when the usual drugs fail:
- nonspecific beta-agonists, injected or inhaled (epinephrine, isoetharine, isoproterenol, metaproterenol);
- anticholinergics, IV or nebulized, with systemic effects (glycopyrrolate, atropine);
- methylxanthines (theophylline, aminophylline);
- inhalation anesthetics that have a bronchodilatory effect (isoflurane, halothane, enflurane);
- the dissociative anaesthetic ketamine, often used in endotracheal tube induction
- magnesium sulfate, intravenous; and
- intubation and mechanical ventilation, for patients in or approaching respiratory arrest.
Alternative and complementary medicine
Many asthmatics, like those who suffer from other chronic disorders, use alternative treatments; surveys show that roughly 50% of asthma patients use some form of unconventional therapy.[34][35] There are little data to support the effectiveness of most of these therapies. A Cochrane systematic review of acupuncture for asthma found no evidence of efficacy.[36] A similar review of air ionisers found no evidence that they improve asthma symptoms or benefit lung function; this applied equally to positive and negative ion generators.[37] A study of "manual therapies" for asthma, including osteopathic, chiropractic, physiotherapeutic and respiratory therapeutic maneuvers, found no evidence to support their use in treating asthma;[38] these manoeuvres include various osteopathic and chiropractic techniques to "increase movement in the rib cage and the spine to try and improve the working of the lungs and circulation"; chest tapping, shaking, vibration, and the use of "postures to help shift and cough up phlegm." On the other hand, one meta-analysis found that homeopathy has a potentially mild benefit in reducing symptom intensity;[39] however, the number of patients involved in the analysis was small, and subsequent studies have not supported this finding.[40] Several small trials have suggested some benefit from various yoga practices, ranging from integrated yoga programs[41] "yogasanas, Pranayama, meditation, and kriyas"to sahaja yoga,[42] a form of meditation.
The Buteyko method, a Russian therapy based on breathing exercises, has been investigated with mixed degrees of effect shown. A randomized, controlled trial of just 39 patients in 1998, suggested that it may moderately reduce the need for beta-agonists among asthmatics, but found no objective improvement in lung function.[43] Whilst a trial in New Zealand, 2003, showed reduced beta-agonist medication by 94% and inhaled steroid by 34% after just six weeks.[44]
Given that some research has identified a negative association between helminth infection (hookworm) and asthma and hay fever, some have suggested that hookworm infestation, although not medically sanctioned, would cure asthma. There is anectdotal evidence to support this.[45]
Prognosis
The prognosis for asthmatics is good, especially for children with mild disease. For asthmatics diagnosed during childhood, 54% will no longer carry the diagnosis after a decade. The extent of permanent lung damage in asthmatics is unclear. Airway remodelling is observed, but it is unknown whether these represent harmful or beneficial changes.[6] Although conclusions from studies are mixed, most studies show that early treatment with glucocorticoids prevents or ameliorates decline in lung function as measured by several parameters.[46] For those who continue to suffer from mild symptoms, corticosteroids can help most to live their lives with few disabilities. The mortality rate for asthma is low, with around 6000 deaths per year in a population of some 10 million patients in the United States.[5] Better control of the condition may help prevent some of these deaths.
Epidemiology

More than 6% of children in the United States have been diagnosed with asthma, a 75% increase in recent decades. The rate soars to 40% among some populations of urban children. Asthma is usually diagnosed in childhood. The risk factors for asthma include:
- a personal or family history of asthma or atopy;
triggers (see Pathophysiology above);
premature birth or low birth weight;
viral respiratory infection in early childhood;
maternal smoking;
being male, for asthma in prepubertal children; and
being female, for persistence of asthma into adulthood.
There is a reduced occurrence of asthma in people who were breast-fed as babies. Current research suggests that the prevalence of childhood asthma has been increasing. According to the Centers for Disease Control and Prevention's National Health Interview Surveys, some 9% of US children below 18 years of age had asthma in 2001, compared with just 3.6% in 1980 (see figure). The World Health Organization (WHO) reports that some 8% of the Swiss population suffers from asthma today, compared with just 2% some 2530 years ago.[47] Although asthma is more common in affluent countries, it is by no means a problem restricted to the affluent; the WHO estimate that there are between 15 and 20 million asthmatics in India. In the U.S., urban residents, Hispanics, and African Americans are affected more than the population as a whole. Globally, asthma is responsible for around 180,000 deaths annually.[47]
On the remote South Atlantic island Tristan da Cunha, 50% of the population are asthmatics due to heredity transmission of a mutation in the gene CC16.
Socioeconomic factors
The incidence of asthma is higher among low-income populations within a society (even though it is more common in developed countries than developing countries), which in the western world are disproportionately minority, and more likely to live near industrial areas. Additionally, asthma has been strongly associated with the presence of cockroaches in living quarters, which is more likely in such neighbourhoods.[48]
The quality of asthma treatment varies along racial lines, likely because many low-income people cannot afford health insurance and because there is still a correlation between class and race. For example, black Americans are less likely to receive outpatient treatment for asthma despite having a higher prevalence of the disease. They are much more likely to have emergency room visits or hospitalization for asthma, and are three times as likely to die from an asthma attack compared to whites. The prevalence of "severe persistent" asthma is also greater in low-income communities compared with communities with better access to treatment.[49][50]
Asthma and athletics
Asthma appears to be more prevalent in athletes than in the general population. One survey of participants in the 1996 Summer Olympic Games showed that 15% had been diagnosed with asthma, and that 10% were on asthma medication.[51] These statistics have been questioned on at least two bases. Persons with mild asthma may be more likely to be diagnosed with the condition than others because even subtle symptoms may interfere with their performance and lead to pursuit of a diagnosis. It has also been suggested that some professional athletes who do not suffer from asthma claim to do so in order to obtain special permits to use certain performance-enhancing drugs.
There appears to be a relatively high incidence of asthma in sports such as cycling, mountain biking, and long-distance running, and a relatively lower incidence in weightlifting and diving. It is unclear how much of these disparities are from the effects of training in the sport, and from self-selection of sports that may appear to minimize the triggering of asthma.[51][52]
In addition, there exists a variant of asthma called exercise-induced asthma that shares many features with allergic asthma. It may occur either independently, or concurrent with the latter. Exercise studies may be helpful in diagnosing and assessing this condition.
References
- ^ Zhao J, Takamura M, Yamaoka A, Odajima Y, Iikura Y. Altered eosinophil levels as a result of viral infection in asthma exacerbation in childhood. J Pediatr Allergy Immunol. 2002 Feb;13(1):47-50. PMID 12000498
- ^ Lilly CM. Diversity of asthma: Evolving concepts of pathophysiology and lessons from genetics. J Allergy Clin Immunol. 2005;115(4 Suppl):S526-31. PMID 15806035
- ^ Marketos SG, Ballas CN. Bronchial asthma in the medical literature of Greek antiquity. J Asthma. 1982;19(4):263-9. PMID 6757243
- ^ Rosner F. Moses Maimonides' treatise on asthma. Thorax. 1981;36:245-251. PMID 7025335
- ^ a b c McFadden ER, Jr. Asthma. In Kasper DL, Fauci AS, Longo DL, et al (eds). Harrison's Principles of Internal Medicine (16th Edition), pp. 1508-1516. New York: McGraw-Hill;2004.
- ^ a b Maddox L, Schwartz DA. The Pathophysiology of Asthma. Annu. Rev. Med. 2002, 53:477-98. PMID 11818486
- ^ Jenkins C, Costello J, Hodge L. Systematic review of prevalence of aspirin induced asthma and its implications for clinical practice. BMJ 2004;328:434. PMID 14976098
- ^ Nemery B, Hoet PH, Nowak D. Indoor swimming pools, water chlorination and respiratory health. Eur Respir J. 2002;19(5):790-3. PMID 12030714
- ^ Szentivanyi, Andor (1968). "The Beta Adrenergic Theory of the Atopic Abnormality in Asthma".
- ^ Lockey, Richard, In lasting tribute: Andor Szentivanyi, MD. J. Allergy and Clinical Immunology, January, 2006
- ^
(1993) "The in
vitro effect of Imunnoglobulin E {IgE} on cyclic AMP
concentrations in A549 human pulmonary epithelial
cells with or without beta adrenergic stimulation".
J. Allergy Clin Immunol. 91: 379.
- Part of Abstracts from:
(1993) "50th Anniversary of the American Academy of Allergy and Immunology. 49th Annual Meeting. Chicago, Illinois, March 12-17, 1993. Abstracts.". J Allergy Clin Immunol 91 (1 Pt 2): 141-379. PMID 8421135. - ^ (2001) Kowalak JP, Hughes AS et al (eds) Professional Guide To Diseases, 7th ed., Springhouse.
- ^ Lockey, Richard F. (2006-04-28). Anaphylaxis: Synopsis. Allergic Diseases Resource Center. World Allergy Organization. Retrieved on September 23, 2006.
- ^ Ouellette, J. J., C. E. Reed (March 1967). "The effect of partial beta adrenergic blockade on the bronchial response of hay fever subjects to ragweed aerosol.". Journal of Allergy 39 (3): 160-6. PubMed.
- ^ Fraser, Claire M., J. Craig Venter (May 14, 1980). "The synthesis of beta-adrenergic receptors in cultured human lung cells: induction by glucocorticoids." (PDF). Biochemical and Biophysical Research Communications 94 (1): 390-397. DOI:10.1016/S0006-291X(80)80233-6. PubMed. Retrieved on 2006-09-23.
- ^ Terttu HH, Leinonen M, Nokso-Koivisto J, Korhonen T, Raty R, He Q, Hovi T, Mertsola J, Bloigu A, Rytila P, Saikku P (2006). "Non-random distribution of pathogenic bacteria and viruses in induced sputum or pharyngeal secretions of adults with stable asthma". Thorax. PMID 16517571.
- ^ a b Richeldi L, Ferrara G, Fabbri LM, Lasserson TJ, Gibson PG (2005). "Macrolides for chronic asthma". Cochrane Database Syst Rev (4): CD002997. PMID 16235309.
- ^ Pasternack R, Huhtala H, Karjalainen J (2005). "Chlamydophila (Chlamydia) pneumoniae serology and asthma in adults: a longitudinal analysis". J Allergy Clin Immunol 116 (5): 1123-8. PMID 16275386.
- ^ Ronchetti R, Biscione GL, Ronchetti F, Ronchetti MP, Martella S, Falasca C, Casini C, Barreto M, Villa MP (2005). "Why Chlamydia pneumoniae is associated with asthma and other chronic conditions? Suggestions from a survey in unselected 9 yr old schoolchildren". Pediatr Allergy Immunol 16 (2): 145-50. PMID 15787872.
- ^ University of Michigan Health System (May 25, 2005). Breathing disorders during sleep are common among asthmatics, may help predict severe asthma. Press release. Retrieved on 2006-09-23.
- ^ Basner, Robert C. (2006-07-25). Asthma and OSA. ASAA Resources > Publications. American Sleep Apnea Association. Retrieved on September 23, 2006.
- ^ Leggett, Julian J., Brian T. Johnston, Moyra Mills, Jackie Gamble, and Liam G. Heaney (April 2005). "Prevalence of Gastroesophageal Reflux in Difficult Asthma". Chest 127 (4): 1227-1231. PubMed. Retrieved on 2006-09-23.
- ^ American Journal of Respiratory and Critical Care Medicine 1995;151:969-74.
- ^ Thomson NC, Spears M. The influence of smoking on the treatment response in patients with asthma. Curr Opin Allergy Clin Immunol. 2005;5(1):57-63. PMID 15643345
- ^ Eisner MD, Yelin EH, Katz PP, et al. Exposure to indoor combustion and adult asthma outcomes: environmental tobacco smoke, gas stoves, and woodsmoke. Thorax. 2002;57(11):973-8. PMID 12403881
- ^ a b National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the Diagnosis and Management of Asthma. National Institutes of Health pub no 97-4051. Bethesda, MD, 1997. (PDF)
- ^ British Thoracic Society & Scottish Intercollegiate Guidelines Network (SIGN). British Guideline on the Management of Asthma. Guideline No. 63. Edinburgh:SIGN; 2004. (HTML, Full PDF, Summary PDF)
- ^ Cromie, William J.. "Researchers uncover cause of asthma", Harvard University Gazette, Harvard News Office, 2006-03-16. Retrieved on 2006-09-23.
- ^ a b Hendeles L, Marshik PL, et al. Response to nonprescription epinephrine inhaler during nocturnal asthma. Ann Allergy Asthma Immunol. 2005 Dec;95(6):530-4. PMID 16400891
- ^ Rodrigo GJ, Nannini LJ. Comparison between nebulized adrenaline and beta2 agonists for the treatment of acute asthma. A meta-analysis of randomized trials. Am J Emerg Med. 2006 Mar;24(2):217-22. PMID 16490653
- ^ Serevent Diskus, Advair Diskus, and Foradil Information (Long Acting Beta Agonists) - Drug information. FDA (2006-03-03).
- ^ Ramanujan, Krishna (2006-06-09). Common asthma inhalers cause up to 80 percent of asthma-related deaths, Cornell and Stanford researchers assert. Cornell Chronicle Online. Cornell News Service. Retrieved on 2006-09-23.
- ^ Rodrigo GJ, Rodrigo C, Hall JB. Acute asthma in adults: a review. Chest. 2004;125(3):1081-102. PMID 15006973
- ^ Blanc PD, Trupin L, Earnest G, et al. Alternative therapies among adults with a reported diagnosis of asthma or rhinosinusitis: data from a population-based survey. Chest. 2001;120(5):1461-7. PMID 11713120
- ^ Shenfield G, Lim E, Allen H. Survey of the use of complementary medicines and therapies in children with asthma. J Paediatr Child Health. 2002;38(3):252-7. PMID 12047692
- ^ McCarney RW, Brinkhaus B, Lasserson TJ, et al. Acupuncture for chronic asthma. Cochrane Database Syst Rev. 2004;(1):CD000008. PMID 14973944
- ^ Blackhall K, Appleton S, Cates CJ. Ionisers for chronic asthma. Cochrane Database Syst Rev. 2003;(3):CD002986 PMID 12917939
- ^ Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database Syst Rev. 2005;(2):CD001002. PMID 15846609
- ^ Reilly D, Taylor MA, Beattie NG, et al. Is evidence for homoeopathy reproducible? Lancet. 1994;344(8937):1601-6. PMID 7983994
- ^ White A, Slade P, Hunt C, et al. Individualised homeopathy as an adjunct in the treatment of childhood asthma: a randomised placebo controlled trial. Thorax. 2003;58(4):317-21. PMID 12668794
- ^ Nagendra HR, Nagarathna R. An integrated approach of yoga therapy for bronchial asthma: a 3-54-month prospective study. J Asthma. 1986;23(3):123-37. PMID 3745111
- ^ Manocha R, Marks GB, Kenchington P, et al. Sahaja yoga in the management of moderate to severe asthma: a randomised controlled trial. Thorax. 2002;57(2):110-5. PMID 11828038
- ^ Bowler SD, Green A, Mitchell CA. Buteyko breathing techniques in asthma: a blinded randomised controlled trial. Med J Aust. 1998;169(11-12):575-8. PMID 9887897
- ^ McHugh P, Aitcheson F, Duncan B, Houghton F. Buteyko Breathing Technique for asthma: an effective intervention. NZ Med J. 2003;116:1187 PMID 16718299
- ^ "Worm infestation 'beats asthma'", BBC News, 2001-11-02.
- ^ Beckett PA, Howarth PH. Pharmacotherapy and airway remodelling in asthma? Thorax. 2003;58(2):163-74. PMID 12554904
- ^ a b World Health Organization. Bronchial asthma: scope of the problem. Retrieved on 2005-08-23.
- ^ Patient/Public Education: Fast Facts - Asthma Demographics/Statistics. American Academy of Allergy Asthma & Immunology. Retrieved on 2006-05-02.
- ^ National Heart, Lung, and Blood Institute (May 2004). Morbidity & Mortality: 2004 Chart Book On Cardiovascular, Lung, and Blood Diseases. National Institutes of Health.
- ^ National Center for Health Statistics (07 April 2006). Asthma Prevalence, Health Care Use and Mortality, 2002. Centers for Disease Control and Prevention.
- ^ a b Weiler JM, Layton T, Hunt M. Asthma in United States Olympic athletes who participated in the 1996 Summer Games. J Allergy Clin Immunol. 1998;102(5):722-6. PMID 9819287
- ^ Helenius I, Haahtela T. Allergy and asthma in elite summer sport athletes. J Allergy Clin Immunol. 2000;106(3):444-52 PMID 10984362
External links
- National Heart, Lung, and Blood Institute Asthma U.S. NHLBI Information for Patients and the Public page.
- National Heart, Lung, and Blood Institute Asthma U.S. NHLBI Information for Health Professionals page.
- MedLinePlus: Asthma a U.S. National Library of Medicine page.
- American Academy of Allergy, Asthma, and Immunology a U.S. organization of medical professionals with a special interest in treating and researching conditions such as allergic rhinitis, asthma, atopic dermatitis/eczema, and anaphylaxis.
- Asthma UK a patient-oriented site with information on asthma and ways that UK residents can help improve asthma-related policy.
- Asthma Foundation of Queensland Information and education for Australian asthma sufferers.
- Children's Hospital & Regional Medical Center Allergies, Asthma & Immune System A Seattle, Washington hospital website with patient-oriented videos on asthma and the immune system.
- Case Studies in Environmental Medicine (CSEM): Environmental Triggers of Asthma Agency for Toxic Substances and Disease Registry, U.S. Department of Health and Human Services.
- Asthma as Neurogenic Inflammatory Disease Neurogenic aspects of asthma. Pathophysiological links with other inflammatory disorders.
