


 216.73.216.110
216.73.216.110 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 216.73.xxx.xxx
216.73.xxx.xxx
 Server Time:
Server Time:
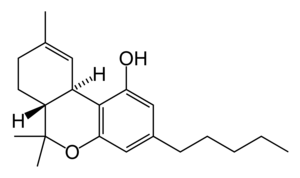
| Tetrahydrocannabinol (THC) | |
|---|---|
| Chemical name | (−)-(6aR,10aR)-6,6,9-trimethyl- 3-pentyl-6a,7,8,10a-tetrahydro- 6H-benzo[c]chromen-1-ol |
| Chemical formula | C21H30O2 |
| Molecular mass | 314.46 g/mol |
| Glass transition | 9.3 °C |
| Boiling point | 155-157 °C (vacuum, 0.07 mbar) |
| Solubility (water) | 2.8 mg/L (23 °C) |
| Solubility (saline) | 0.77 mg/L (NaCl, 0.15 M) |
| pKa | 10.6 |
| log P | 3.78 (water @ pH 7 / octanol) |
| CAS number | 1972-08-3 |
| SMILES | CCCCCC(C=C1O)=CC2=C1[C@]3([H]) [C@](C(C)(C)O2)([H])CCC(C)=C3 |
|
|
Tetrahydrocannabinol, also known as THC, Δ9-THC, Δ9-tetrahydrocannabinol (delta-9-tetrahydrocannabinol), Δ¹-tetrahydrocannabinol (using an older numbering scheme), or dronabinol, is the main psychoactive substance found in the Cannabis plant. It was isolated by Raphael Mechoulam and Yechiel Gaoni from the Weizmann Institute in Rehovot, Israel in 1964. In pure form it is a glassy solid when cold and becomes viscous and sticky if warmed. THC has a very low solubility in water, but a good solubility in most organic solvents such as ethanol or hexane. As in the case of nicotine and caffeine, THC's most likely function in Cannabis is to protect the plant from herbivores or pathogens [1].
Contents |
Pharmacology
Its pharmacological actions are the result of its binding to the cannabinoid receptor CB1, located in the brain. The presence of these specialized receptors in the brain implied to researchers that endogenous cannabinoids were manufactured by the body, so the search began for a substance normally manufactured in the brain that binds to these receptors, the so-called natural ligand or agonist, leading to the eventual discovery of anandamide, 2 arachidonyl glyceride (2-AG) and other related compounds. This story resembles the discovery of the endogenous opiates (endorphins, enkephalins, and dynorphin), after the realization that morphine and other opiates bound to specific receptors in the brain.
THC has analgesic effects even at low doses that do not cause a "high", and cannabis was once commonly used to treat pain. Other effects include: relaxation; euphoria; altered space-time perception; alteration of visual, auditory, and olfactory senses; disorientation; fatigue; and appetite stimulation. It also has anti-emetic properties, and also may reduce aggression in certain subjects.
Toxicity
THC has a LD50 value of 1270 mg/kg (male rats) and 730 mg/kg (female rats) administered orally dissolved in sesame oil.
If this were scaled up to an adult human, the lethal dose would be between approximately 50 and 86 g for a 68 kg (150 lb) female or male person respectively. This would be equivalent to 1-1.8 kg of marijuana with a 5% THC content (roughly average) taken orally (much more if smoked). It is important to note, however, that toxicity studies in animal models do not necessarily correlate to human toxicity. THC receptor distribution in the rat CNS is different from that of humans, meaning that there is the significant possibility that toxicity in humans varies from the published animal LD50 studies. There has never been a documented fatality from marijuana or THC overdose.
Studies of the distribution of the cannabinoid receptors in the brain explain why THC's toxicity is so low (i.e., the LD50 of the compound is so large): parts of the brain that control vital functions such as respiration do not have many receptors, so they are relatively unaffected even by doses larger than could ever be ingested under any normal conditions.
Research
A number of studies indicate that THC may provide medical benefits for cancer and AIDS patients by increasing appetite and decreasing nausea, and by blocking the spread of some cancer-causing Herpes simplex viruses. It has been shown to assist some glaucoma patients by reducing pressure within the eye, and is used in the form of cannabis by a number of multiple sclerosis patients to relieve the spasms associated with their condition.
Studies also indicate a variety of negative effects associated with constant, long-term use, including short-term memory loss. However, other studies have refuted this, claiming the MRIs of long term users show little or no difference to MRIs of the non-using control group. The long-term effects of THC on humans have been disputed because its status as an illegal drug makes research difficult.
Preliminary research on synthetic THC has been conducted on patients with Tourette syndrome, with results suggesting that it may help in reducing nervous tics and urges by a significant degree. Animal studies suggested that Marinol and nicotine could be used as an effective adjunct to neuroleptic drugs in treating TS. Research on twelve patients showed that Marinol reduced tics with no significant adverse effects. A six-week controlled study on 24 patients showed the patients taking Marinol had a significant reduction in tic severity without serious adverse effects. Seven patients dropped out or had to be excluded from the study, one due to adverse side-effects. More significant reduction in tic severity was reported with longer treatment. No detrimental effects on cognitive functioning and a trend towards improvement in cognitive functioning were reported during and after treatment. Marinol's usefulness as a treatment for TS cannot be determined until/unless longer controlled studies on larger samples are undertaken.
Recent research has shown that many adverse side effects, generally known as the "stoner" stereotype, fail to hold up to the scientific method. Recent studies with synthetic cannabinoids show that activation of CB1 receptors can facilitate neurogeneration, as well as neuroprotection, and can even help prevent natural neural degredation from neurodegenerative diseases such as MS, Parkinson's, and Alzheimer's. This, along with research into the CB2 receptor (throughout the immune system), has given the case for medical marijuana more support.
THC, the main active component in marijuana, may protect the brain from the ravages of Alzheimer's disease, U.S. scientists reported. In lab experiments release on 10/09/2006, investigators from Scripps Research Institute in La Jolla, Calif., found THC appears to block an enzyme in the brain that causes plaques to form better than currently approved drugs.
Synthetic THC
Synthetic THC, also known under the substance name dronabinol, is available as a prescription drug (under the trade name Marinol) in several countries including the USA, The Netherlands, and Germany. In the United States, Marinol is a Schedule III drug, available by prescription, considered to be non-narcotic and to have a low risk of physical or mental dependence. Efforts to get cannabis rescheduled as analogous to Marinol have not succeeded thus far. As a result of the rescheduling of Marinol from Schedule II to Schedule III, refills are now permitted for this substance. Marinol has been approved by the FDA in the treatment of anorexia in AIDS patients, as well as for refractory nausea and vomiting of patients undergoing chemotherapy.
An analog of dronabinol, nabilone, is available commercially in Canada under the trade name Cesamet, manufactured by Valeant. Cesamet has also received FDA approval for future availability in the United States and is a Schedule II drug.
In April 2005, Canadian authorities approved the marketing of Sativex, a mouth spray for multiple sclerosis to alleviate pain. Sativex contains tetrahydrocannabinol together with cannabidiol. It is marketed in Canada by GW Pharmaceuticals, being the first cannabis-based prescription drug in the world.
See also
References
External links
- Scientific American Marijuana research
- Erowid Compounds found in Cannabis sativa.
- Machinery of the "marijuana munchies"
