


 216.73.216.110
216.73.216.110 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 216.73.xxx.xxx
216.73.xxx.xxx
 Server Time:
Server Time:
 |
|
|
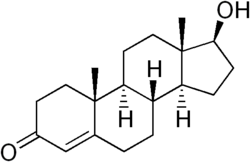
Testosterone
|
|
| Systematic (IUPAC) name | |
| 17b-hydroxy-4-androsten-3-one | |
| Identifiers | |
| CAS number | 58-22-0 |
| ATC code | G03BA03 |
| PubChem | 6013 |
| Chemical data | |
| Formula | C19H28O2 |
| Mol. weight | 288.43 |
| Physical data | |
| Melt. point | 155-156 °C (-94 °F) |
| Spec. rot | +110,2° |
| SEC Combust | −11080 kJ/mol |
| Pharmacokinetic data | |
| Metabolism | Liver, Testis and Prostate |
| Half life | 1-12 days |
| Excretion | Urine |
| Therapeutic considerations | |
| Pregnancy cat. | X (USA), Teratogenic effects |
| Legal status | Schedule III (USA) Schedule IV (Canada) |
| Routes | Intramuscular injection, transdermal (cream, gel, or patch), oral, sub-'Q' pellet |
Testosterone is a steroid hormone from the androgen group. Testosterone is primarily secreted in the testes of males and the ovaries of females although small amounts are secreted by the adrenal glands. It is the principal male sex hormone and an anabolic steroid. In both males and females, it plays key roles in health and well-being. Examples include enhanced libido, energy, immune function, and protection against osteoporosis. On average, the adult male body produces about twenty times the amount of testosterone that an adult female's body does[1].
Contents |
Sources of testosterone
Like other steroid hormones, testosterone is derived from cholesterol. The largest amounts of testosterone are produced by the testes in men, but it is also synthesized in smaller quantities in women by the thecal cells of the ovaries, by the placenta, as well as by the zona reticularis of the adrenal cortex in both sexes.
In the testes, testosterone is produced by the Leydig cells. The male generative glands also contain Sertoli cells which require testosterone for spermatogenesis. Like most hormones, testosterone is supplied to target tissues in the blood where much of it is transported bound to a specific plasma protein, sex hormone binding globulin (SHBG).
Some drugs specifically target testosterone as a way of treating certain conditions. For example, finasteride inhibits the conversion of testosterone into dihydrotestosterone (DHT), a metabolite which is more potent than testosterone. By lowering the levels of dihydrotestosterone, finasteride may be used for various conditions associated with androgens, such as benign prostatic hyperplasia (BPH) and androgenetic alopecia (male-pattern baldness).
Mechanism of effects
The effects of testosterone in humans and other vertebrates occur by way of two main mechanisms: by activation of the androgen receptor (directly or as DHT), and by conversion to estradiol and activation of certain estrogen receptors.
Free testosterone (T) is transported into the cytoplasm of target tissue cells, where it can bind to the androgen receptor, or can be reduced to 5α-dihydrotestosterone (DHT) by the cytoplasmic enzyme 5α-reductase(5-alfa-reduktas). DHT binds to the same androgen receptor even more strongly than T, so that its androgenic potency is about 2.5 times that of T. The T-receptor or DHT-receptor complex undergoes a structural change that allows it to move into the cell nucleus and bind directly to specific nucleotide sequences of the chromosomal DNA. The areas of binding are called hormone response elements (HREs), and influence transcriptional activity of certain genes, producing the androgen effects. It is important to note that if there is a too low amount of 5α-reductase(5-alfa-reduktas), the body (of a human) will -continue- growing into a female with testicles.
Androgen receptors occur in many different vertebrate body system tissues, and both males and females respond similarly to similar levels. Greatly differing amounts of testosterone prenatally, at puberty, and throughout life account for a large share of biological differences between males and females.
The bones and the brain are two important tissues in humans where the primary effect of testosterone is by way of aromatization to estradiol. In the bones, estradiol accelerates maturation of cartilage into bone, leading to closure of the epiphyses and conclusion of growth. In the central nervous system, testosterone is aromatized to estradiol. Estradiol rather than testosterone serves as the most important feedback signal to the hypothalamus (especially affecting LH secretion). In many mammals, prenatal or perinatal "masculinization" of the sexually dimorphic areas of the brain by estradiol derived from testosterone programs later male sexual behavior.
Testerone is a predominantly male hormone, though females do
produce certain amounts of it. The primary female hormone is
estrogen and males also produce certain amounts of this
hormone. Testosterone causes the appearance of male traits
(i.e deepening voice, pubic and facial hairs, muscular
build, etc.)
Effects of testosterone on humans
In general, androgens promote protein synthesis and growth of those tissues with androgen receptors. Testosterone effects can be classified as virilizing and anabolic effects, although the distinction is somewhat artificial, as many of the effects can be considered both. Anabolic effects include growth of muscle mass and strength, increased bone density and strength, and stimulation of linear growth and bone maturation. Virilizing effects include maturation of the sex organs, particularly the penis and the formation of the scrotum in fetuses, and after birth (usually at puberty) a deepening of the voice, growth of the beard and axillary hair. Many of these fall into the category of male secondary sex characteristics.
Testosterone effects can also be classified by the age of usual occurrence. For postnatal effects in both males and females, these are mostly dependent on the levels and duration of circulating free testosterone.
Most of the prenatal androgen effects occur between 7 and 12 weeks of gestation.
- Genital virilization (midline fusion, phallic urethra, scrotal thinning and rugation, phallic enlargement)
- Development of prostate and seminal vesicles
Early infancy androgen effects are the least understood. In the first weeks of life for male infants, testosterone levels rise. The levels remain in a pubertal range for a few months, but usually reach the barely detectable levels of childhood by 4-6 months of age. The function of this rise in humans is unknown. It has been speculated that "brain masculinization" is occurring since no significant changes have been identified in other parts of the body.
Early postnatal effects are the first visible effects of rising androgen levels in childhood, and occur in both boys and girls in puberty.
- Adult-type body odour
- Increased oiliness of skin and hair, acne
- Pubarche (appearance of pubic hair)
- Axillary hair
- Growth spurt, accelerated bone maturation
- Fine upper lip and sideburn hair
Advanced postnatal effects begin to occur when androgen has been higher than normal adult female levels for months or years. In males these are normal late pubertal effects, and only occur in women after prolonged periods of excessive levels of free testosterone in the blood.
- Phallic enlargement (including clitoromegaly)
- Increased libido and erection frequency
- Pubic hair extends to thighs and up toward umbilicus
- Facial hair (sideburns, beard, moustache)
- Chest hair, periareolar hair, perianal hair
- Subcutaneous fat in face decreases
- Increased muscle strength and mass
- Deepening of voice
- Growth of the adam's apple
- Growth of spermatogenic tissue in testes, male fertility
- Growth of jaw, brow, chin, nose, and remodeling of facial bone contours
- Shoulders widen and rib cage expands
- Completion of bone maturation and termination of growth. This occurs indirectly via estradiol metabolites and hence more gradually in men than women.
Adult testosterone effects are more clearly demonstrable in males than in females, but are likely important to both sexes. Some of these effects may decline as testosterone levels decline in the later decades of adult life.
- Maintenance of muscle mass and strength
- Maintenance of bone density and strength
- Libido and erection frequency
- Mental and physical energy
Effects of testosterone on the human brain
As testosterone affects the entire body (often by enlargening, such accepted facts such as, men have bigger hearts, lungs, liver etc) the brain is also affected by this "sexual" advancement, the enzyme aromatase converts testosterone into estrogen that is responsible for "masculinization" of the brain in a male fetus. Factors that in any way reduce this key enzyme(aromatase) can result in an individual with male gender, male body but with a "female" brain. There are some differences in a male and female brain (the result of testosterone) a clear difference is the size, the male human brain is on average larger, however in females the (that do not use testosterone as much) the corpus callosum is proportionally larger in females then males. This means that the effect of testosterone is a greater brain volume, however less interwoven brain halves. [2]
Testosterone in athletes
Testosterone may be administered to an athlete in order to improve performance, and is considered to be a form of doping in most sports. There are several application methods for testosterone, including intramuscular injections, transdermal gels and patches, and implantable pellets.
Anabolic steroids (of which testosterone is one) have also been taken to enhance muscle development, strength, or endurance. After a series of scandals and publicity in the 1980s (such as Ben Johnson's improved performance at the 1988 Summer Olympics), prohibitions of anabolic steroid use were renewed or strengthened by many sports organizations. Testosterone and other anabolic steroids were designated a "controlled substance" by the United States Congress in 1990, with the Anabolic Steroid Control Act.[1]
Therapeutic use of testosterone
Testosterone was first isolated from a bull in 1935. There have been many pharmaceutical forms over the years. Forms of testosterone for human administration currently available in North America include injectable (such as testosterone cypionate or testosterone enanthate in oil), oral Andriol, buccal Striant, transdermal skin patches, and transdermal creams or gels Androgel and Testim. In the pipeline are a "roll on" delivery method and a nasal spray.
The original and primary use of testosterone is for the treatment of males who have too little or no natural endogenous testosterone production; males with hypogonadism. Appropriate use for this purpose is legitimate hormone replacement therapy, which maintains serum testosterone levels in the normal range.
However, over the years, as with every hormone, testosterone or other anabolic steroids has also been given for many other conditions and purposes besides replacement, with variable success but higher rates of side effects or problems. Examples include infertility, lack of libido or erectile dysfunction, osteoporosis, penile enlargement, height growth, bone marrow stimulation and reversal of anemia, and even appetite stimulation. By the late 1940s testosterone was being touted as an anti-aging wonder drug (e.g., see Paul de Kruif's The Male Hormone).
To take advantage of its virilizing effects, testosterone is often administered to transmen (female-to-male transsexual and transgender people) as part of the hormone replacement therapy, with a "target level" of the normal male testosterone level. And like-wise, transwomen are sometimes prescribed drugs [anti-androgens] to decrease the level of testosterone in the body and allow for the effects of estrogen to develop.
There is a myth that exogenous testosterone can more or less definitively be used for male birth control. However, the vast majority of physicians will agree that to prescribe exogenous testosterone for this purpose is inappropriate. But perhaps more importantly, many men of first hand found this myth to be untrue or at least, unreliable. This is especially true when exogenous testosterone is used in conjunction with hCG.
Exogenous testosterone supplementation comes with a number of health risks. Fluoxymesterone and methyltestosterone are synthetic derivatives of testosterone. In 2006 it was reported that women taking Estratest, a combination pill including estrogen and methyltestosterone, were at considerably heightened risk of breast cancer.
The "testosterone deficiency" of aging and the andropause controversy
Testosterone levels decline gradually with age in men. The clinical significance of this decrease is debated. There is disagreement about if and when to treat aging men with testosterone replacement therapy. The American Society of Andrology's position is that testosterone therapy "is indicated when both clinical symptoms and signs suggestive of androgen deficiency and decreased testosterone levels are present". The American Association of Clinical Endocrinologists says "Hypogonadism is defined as a free testosterone level that is below the lower limit of normal for young adult control subjects. Previously, age-related decreases in free testosterone were once accepted as normal. Currently, they are not considered normal....Patients with low-normal to subnormal range testosterone levels warrant a clinical trial of testosterone." [2]
There isn't total agreement on the threshold of testosterone value below which a man would be considered hypogonadal. Testosterone can be measured as "free" (that is, bioavailable and unbound) or more commonly, "total" (including the percentage which is chemically bound and unavailable). In the United States, male total testosterone levels below 200 to 300 ng/dl from a morning sample are generally considered low. However these numbers are typically not age-adjusted, but based on an average of a test group which includes elderly males with low testosterone levels. Therefore a value of 300 ng/dl might be normal for a 90 year old male, but not normal for a 30 year old. Identification of inadequate testosterone in an aging male by symptoms alone can be difficult. The signs and symptoms are non-specific, and might be confused with normal aging characteristics, such as loss of muscle mass and bone density, decreased physical endurance, decreased memory ability and loss of libido.
Replacement therapy can take the form of injectable depots, transdermal patches and gels, subcutaneous pellets and oral therapy. Adverse effects of testosterone supplementation include minor side effects such as acne and oily skin, and more significant complications such as increased hematocrit, exacerbation of sleep apnea and acceleration of pre-existing prostate cancer growth. Exogenous testosterone also causes suppression of spermatogenesis and can lead to infertility.[3] It is recommended that physicians screen for prostate cancer with a digital rectal exam and PSA (prostate specific antigen) level prior to initiating therapy, and monitor hematocrit and PSA levels closely during therapy.
Large scale trials to assess the efficiency and long-term safety of testosterone are still lacking. Many caution against embracing testosterone replacement therapy because of lessons from the female hormone replacement therapy trials, where initially promising results were later refuted by larger studies.
Synthesis
Testosterone is synthesized from pregnenolone, which is the precursor of all steroid hormones and is made from cholesterol by a series of enzymatic reactions. Two pathways are possible, In the delta-5 pathway, pregnenolone is converted to DHEA to androstenedione.
In the delta-4 pathway there is hydroxylation of C-17 of progesterone, to yield 17α-hydroxyprogesterone. The side chain is then cleaved to form androstenedione. Androstenedione is the immediate precursor to testosterone.
The keto group on C-17 is reduced to an alcohol to yield testosterone. Testosterone is a potential precursor of estradiol.
Zinc supplementation is known to result in increased levels of testosterone synthesis, especially in those who are zinc deficient. Zinc is critical to the proper function of steroid receptors (see zinc finger) and plays a vital role as a cofactor to many enzymes which is the likely mechanism for its effect on testosterone synthesis.
Notes
- ^ Williams textbook of endocrinology, Jean D. Wilson pp. 535, 887
- ^ Mark Solms & Oliver Turnbull - The brain and the inner world'.
- ^ "Contraceptive efficacy of testosterone-induced azoospermia in normal men". Lancet. PubMed.
