


 216.73.216.110
216.73.216.110 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 222.253.xxx.xx
222.253.xxx.xx
 Server Time:
Server Time:
 |
|
|
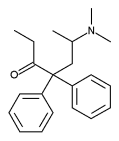
Methadone
|
|
| Systematic (IUPAC) name | |
| 6-dimethylamino-4,4-diphenyl-heptan-3-one | |
| Identifiers | |
| CAS number | 76-99-3 |
| ATC code | N02AC52 N07BC02, R05DA06 |
| PubChem | 4095 |
| DrugBank | APRD00485 |
| Chemical data | |
| Formula | C21H27NO |
| Mol. weight | 309.445 g/mol |
| Pharmacokinetic data | |
| Bioavailability | 40-80(-92) |
| Metabolism | Hepatic |
| Half life | 24-36 hrs. |
| Excretion | Urine, Test by specific gravity and bilirubin |
| Therapeutic considerations | |
| Pregnancy cat. | Reduction of oxygen to unborn child due to depression of breathing |
| Legal status | Class A(UK) Schedule II(US) |
| Dependence Liability | Moderate |
| Routes | oral, intravenous |
Methadone is a synthetic opioid, used medically as an analgesic and in the treatment of narcotic addiction. It was first brought to market by the pharmaceutical company Eli Lilly and Company.
Contents |
History
Methadone/dolophine, was first synthesized in 1937 by German scientists Max Bockmühl and Gustav Ehrhart at IG Farben (Hoechst-Am-Main) during their search for an analgesic that would be easier to use during surgery (and less potentially addictive, post-op) than morphine. Methadone is a Schedule II drug under the Single Convention on Narcotic Drugs[1].
On September 11, 1941 Bockmühl and Ehrhart filed an application for a patent for a synthetic substance they called Hoechst 10820 or polamidon and whose structure had no relation to morphine or the opioid alkaloids (Bockmühl and Ehrhart, 1949). Although chemically unlike morphine or heroin, methadone also acts on the opioid receptors and thus produces many of the same effects. Chemically, methadone is the simplest of the opioids.
Methadone was introduced into the United States in 1947 by Eli Lilly and Company as an analgesic (They gave it the trade name Dolophine,® which is now registered to Roxane Laboratories). Since then, it has been best known for its use in treating narcotic addiction, though it is also used in managing chronic pain due to its long duration of action and very low cost. In late 2004, the cost of a one-month supply of methadone was $20, as compared to an equivalent analgesic amount of Demerol at $120. The old name Dolophine comes from the German Dolphium. The name derives from the Latin dolor which means "pain" and phine which means "end".
Methadone (as Dolophine) was first manufactured in the USA by Mallinckrodt pharmaceuticals, a St. Louis-based subsidiary of the Tyco International corporation. Mallinckrodt held the patent up until the early 1990s. Today a number of pharmaceutical companies produce and distribute methadone. However, the major producer remains Mallinckrodt. Mallinckrodt sells bulk methadone to most of the producers of generic preparations and also distributes its own brand name product in the form of tablets, dispersable tablets and oral concentrate under the name Methadose in the United States.
Generally, one will only hear "dolophine" used by older addicts who used the product in the 1960s and 1970s. Medical professionals who believe that dolophine is the generic name for methadone, when actually it is the reverse, may also use the old brand name. A persistent but untrue urban legend claims that the trade name "Dolophine" was coined in tribute to Adolf Hitler by its German creators, and it is sometimes even claimed that the drug was originally named "adolphine" or "adolophine". The claim is still presented as fact by Church of Scientology literature [2] and was repeated by actor and vocal Scientologist Tom Cruise in a 2005 Entertainment Weekly interview. However, as the magazine pointed out, this isn't true: the name "Dolophine" was in fact created after the war by the American branch of Eli Lilly [3], and the name "Adolphine" (never an actual name of the drug) was created in the United States in the early 1970s.[4]
Pharmacology
Methadone has a slow metabolism and very high lipid solubility, making it longer lasting than morphine-based drugs. Methadone has a typical half-life of 24-36 hours, permitting the administration only once a day in heroin detoxification and maintenance programs. The analgesic activity is shorter than the pharmacological halflife; dosing for pain control usually requires multiple doses per day. The most common mode of delivery at a methadone clinic is in an oral solution. Methadone is almost as effective when administered orally as by injection. As with heroin, tolerance and dependence usually develop with repeated doses. Tolerance to the different physiological effects of methadone varies. Tolerance to analgesia usually occurs during the first few weeks of use; whereas with respiratory depression, sedation, and nausea it is seen within approximately 5-7 days. There is no tolerance formed to constipation produced by methadone or other opioids, however, effects may be less severe after time.
Current research shows methadone has a unique affinity for the NMDA (N-methyl-D-aspartic acid) brain receptor. Some researchers propose that NMDA may regulate psychic dependence and tolerance by exhibiting opioid antagonist-like activity. Withdrawal symptoms are generally less acutely severe than those of morphine and heroin at equivalent doses, but are significantly more prolonged: it can last for weeks.
Clinical use
Opioid addiction
Methadone has traditionally been provided to the addiction population in a highly regulated methadone clinic, generally associated with an outpatient department of a hospital. Clinics such as these stem from programs set up during the Nixon administration to combat heroin use, first in Washington, D.C., then nationwide. In addition to obtaining a daily methadone dose, some who go to this type of clinic for addiction treatment may attend some type of psychological counseling for their addiction. Some are required to attend drug addiction programs but many are not.
Methadone is considered to be generally effective in management of heroin addiction and reduction of HIV rates from needle sharing. At proper dosing, methadone usually reduces the appetite for and need to take heroin. However, some heroin addicts report more difficulty in quitting methadone than heroin. While there is much debate over the treatment schedule and duration required, treatment at a methadone maintenance clinic is intended to be for an indefinite duration. Many factors determine the treatment dose schedule, and some follow the philosophy that methadone maintenance treatment is not curative for heroin addiction.
Chronic pain
In recent years, methadone has gained popularity among physicians for the treatment of other medical problems, such as chronic pain. The increased usage comes as doctors search for an opioid drug that can be dosed less frequently than short-acting drugs like morphine or hydrocodone. Another factor in the increased usage is the low cost of methadone. A month's supply will typically have a retail cost of $30-50 in the United States, compared to hundreds of dollars for alternative opioids. Methadone, with its long half-life (and thus long duration of effect) and good oral bioavailability, is a common second-choice drug for pain that doesn't respond to weaker agonists. Some physicians also choose methadone for treating chronic pain in patients who are thought to have a propensity for addiction.
Methadone prescribed for chronic pain is also tied to an increasing number of drug overdose deaths in the United States, more than any other prescription narcotic painkiller.
According to the National Center for Health Statistics, as well as a 2006 series in the Charleston (WV) Gazette[5], medical examiners listed methadone as contributing to 2,992 deaths in 2003, up from 790 in 1999. Approximately 82% of those deaths were listed as accidental- and most deaths involved combinations of methadone with other drugs (especially benzodiazepines).
Data confirms a correlation between increased methadone distribution through pharmacy channels and the rise in methadone associated mortality. This supports the hypothesis that the growing use of oral methadone, prescribed and dispensed for the outpatient management of chronic pain (vs. opioid addiction treatment), explains the dramatic increases in methadone consumption and the growing availability of the drug for diversion to abuse.
More information on methadone associated mortality can be found at Substance Abuse and Mental Health Services Administration (SAMHSA - U.S. Dept. of Health and Human Services).
Efficacy
The efficacy of methadone, whether for heroin addiction or chronic pain, has long been debated. Methadone is a strong opiate that induces analgesia which is indistinguishable from morphine's and other opiate agonists. Regarding addiction, a Cochrane review (neutral organization that examines medical treatments) from 2004 noted, "Methadone is an effective maintenance therapy intervention for the treatment of heroin dependence as it retains patients in treatment and decreases heroin use better than treatments that do not utilise opioid replacement therapy. It does not show statistically significant superior effect on criminal activity." In other words, opiate-dependent patients stayed in methadone programs, but reduction in criminal activity was no greater than that seen in patients treated without methadone. Of course, given the many clients of methadone programs who cease using drugs and live functional lives, the prescription of methadone seems to inarguably lead to a reduction in crime. These studies of criminal activity, however, ignore the many homeless and extremely impoverished who are in methadone programs. Such people cannot cease criminal activity because it is necessary, at least in the circumstances which they are currently in, to remain alive on a day to day basis. In studies of people with access to housing and jobs, the cessation of illegal opiate use (and continuance of legal opiate use) which methadone's prescription provides reduces criminality. In methadone users who continue to use other drugs and who have access to housing and jobs, the problem lies in use of non-opiate drugs. Since methadone use is not a substitute for non-opiate use, this is to be expected.
Worldwide, there has been an explosion of deaths related to methadone. At the same time, there has been a reduction of deaths due to other opiates. This is because methadone prescriptions have increased and other opiate prescriptions have decreased. Methadone has recently come into favor because of its morpine-equivalent analgesia and the longer half-life of methadone which makes blood levels and thus analgesia more stable in patients. Germany noted that one-half of its drug-related deaths were caused in whole or in part by methadone. In 1996, more than twice as many people died from methadone as died from heroin in England. It should be noted that most overdose deaths involving methadone were caused by concurrent use of benzodiazepines or other sedative drugs such as alcohol. Since the increase in deaths due to methadone has not been part of an increase in overall opiate agonist related deaths, it seems that the reason for this increase is simply a trend towards prescribing methadone rather than other opiates. Thus, scare tactics surrounding a upswing in methadone use and deaths are misleading: opiate use always exists. The particular opiate used matters little or not at all. Methadone, heroin, morphine, oxycodone, and others all have nearly identical effects, at least according to users. Thus, when the deaths to one increase the deaths due to another decrease. The amount of users remains stable while the actual opiate in use changes according to availability.
Abuse
Most methadone abuse is perpetrated by friends and family members of people who receive the drug on a prescription basis for medical conditions. "Street Methadone" has a black market value of roughly one U.S. Dollar per Milligram.
Although not common, methadone is encountered on the illicit drug market and has been associated with a number of overdose deaths. "Street Meth" demand comes primarily from opioid addicts unable to get into a legal methadone program, or addicts who have been removed from a methadone program due to some infraction. Methadone is not a common drug of choice because, generally speaking, addicts seeking a high strongly prefer shorter-acting opioids. Studies have shown that the vast majority of methadone diverted to the illicit market comes from pain management prescriptions or theft from factories/shippers and not from maintenance patients.
Similar drugs
Closely related to methadone, the synthetic compound levo-alphacetylmethadol or LAAM (ORLAAM) has an even longer duration of action (from 48 to 72 hours), permitting a reduction in frequency of use. In 1994 it was approved as a treatment of narcotic addiction. Like methadone, LAAM is in Schedule II of the United States Controlled Substances Act. LAAM has since been removed from the US and European markets due to reports of rare cardiac side effects.
Buprenorphine has also been used in the treatment of narcotic addiction. In the UK and many other countries, however, not only buprenorphine and methadone but also diamorphine (heroin) and other opioids may be used for outpatient treatment of opiate addiction, and treatment is generally provided in much less heavily regulated environments than in the United States. A study from Austria indicated that oral morphine provides better results than oral methadone, and studies of heroin maintenance have indicated that a low background dose of methadone combined with heroin maintenance may significantly improve outcomes for less-responsive patients.
Another close relative of methadone is dextropropoxyphene, first marketed in 1957 under the trade name of Darvon. Oral analgesic potency is one-half to one-third that of codeine, with 65 mg approximately equivalent to about 600 mg of aspirin. Dextropropoxyphene is prescribed for relief of mild to moderate pain. Bulk dextropropoxyphene is in Schedule II of the United States Controlled Substances Act, while preparations containing it are in Schedule IV. More than 100 tons of dextropropoxyphene are produced in the United States annually, and more than 25 million prescriptions are written for the products. This narcotic is associated with a number of toxic side effects and is among the top 10 drugs reported by medical examiners in recreational drug use deaths.
Notes
- ^ http://www.incb.org/pdf/e/list/yellow.pdf
- ^ Buttnor, Al. "The Drug Problem: How It CAN be Solved". Freedom Magazine (vol. 4, iss. 1) p. 15. Retrieved Apr. 7, 2006.
- ^ http://www.exchangesupplies.org/publications/methadone_briefing/section1.html
- ^ http://www.indro-online.de/discovery.pdf (PDF format)
- ^ http://www.wvgazette.com/section/Series/The+Killer+Cure
