


 216.73.216.110
216.73.216.110 User Stats:
User Stats:
 Today: 0
Today: 0 Yesterday: 0
Yesterday: 0 This Month: 0
This Month: 0 This Year: 0
This Year: 0 Total Users: 117
Total Users: 117 New Members:
New Members:
 216.73.xxx.xxx
216.73.xxx.xxx
 Server Time:
Server Time:
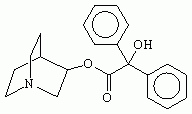
3-quinuclidinyl benzilate (QNB), empirical formula C21H23NO3, full chemical name 1-azabicyclo[2.2.2]oct-3-yl α-hydroxy-α-phenylbenzeneacetate, is an odorless military incapacitating agent. Its NATO code is BZ. The Iraqi incapacitating agent Agent 15 is believed either to be the same as or similar to BZ.
BZ is a glycolate anticholinergic compound related to atropine, scopolamine, hyoscyamine, and other deliriants. Dispersal would be as an aerosolized solid (primarily for inhalation) or as agent dissolved in one or more solvents for ingestion or percutaneous absorption.
Acting as a competitive inhibitor of acetylcholine at postsynaptic and postjunctional muscarinic receptor sites in smooth muscle, exocrine glands, autonomic ganglia, and the brain, BZ decreases the effective concentration of acetylcholine seen by receptors at these sites. Thus, BZ causes peripheral nervous system (PNS) effects that in general are the opposite of those seen in nerve agent poisoning. Central nervous system (CNS) effects include stupor, confusion, and confabulation with concrete and panoramic illusions and hallucinations, and with regression to automatic "phantom" behaviors such as plucking and disrobing.
Physostigmine, which increases the concentration of acetylcholine in synapses and in neuromuscular and neuroglandular junctions, is a specific antidote.
Production of BZ is controlled under schedule 2 of the Chemical Weapons Convention.
Development and military use
Following World War II, the United States military investigated a wide range of possible nonlethal, psychobehavioral chemical incapacitating agents to include psychedelic indoles such as lysergic acid diethylamide (LSD-25) and marijuana derivatives, certain tranquilizers like ketamine or fentanyl, as well as several glycolate anticholinergics. One of the anticholinergic compounds, 3-quinuclidinyl benzilate, was assigned the NATO code BZ and was weaponized at the beginning of the 1960s for possible battlefield use. This agent was reportedly employed by American troops as a counterinsurgency weapon in Vietnam, but supposedly otherwise never saw operational use. It has been rumored that BZ was administered to American troops in order to increase their fighting power and improve their performance, but this rumor is very disputed. This rumor is a major reference point in the film Jacob's Ladder (1990), although the film does not discuss BZ specifically. Destruction of American stockpiles began in 1988 and is now complete.
In February 1998, the British Ministry of Defense released an intelligence report that accused Iraq of having stockpiled large amounts of a glycolate anticholinergic incapacitating agent known as Agent 15. Agent 15 is an alleged Iraqi incapacitating agent that is likely to be chemically either identical to BZ or closely related to it. Agent 15 was reportedly stockpiled in large quantities prior to and during the Persian Gulf War. The combination of anticholinergic PNS and CNS effects aids in the diagnosis of patients exposed to these agents.
Also in 1998, there were allegations that elements of the Yugoslav People's Army used incapacitating agents against fleeing Bosnian refugees in 1995 that caused hallucinations and irrational behavior. [1] Physical evidence of BZ use in Bosnia remains elusive, however.
Sources other than military
BZ and related anticholinergic compounds can be synthesized in clandestine laboratories, but its illicit use is nonexistant, because of its unpleasant effects. 3-quinuclidinyl benzilate, called QNB in the scientific community, is used in pharmacology as a muscarinic receptor antagonist.
Physiochemical characteristics
BZ is odorless. It is stable in most solvents, with a half-life of three to four weeks in moist air; even heat-producing munitions can disperse it. It is extremely persistent in soil and water and on most surfaces. It is also soluble in propylene glycol, DMSO, and other solvents.
Detection and protection
Because BZ is odorless and nonirritating, and because clinical effects are not seen until after a latent period of 30 minutes to 24 hours, exposure could occur without the knowledge of casualties. No currently available field military or civilian detector is designed to disclose the presence of BZ or other anticholinergic compounds in the environment. Confirmation of the exact chemical involved in an incapacitating agent exposure would have to await laboratory analysis of environmental specimens containing the agent. The HEPA filter in the canister of the chemical protective mask prevents exposure of the face and respiratory tract to aerosolized BZ. The chemical protective ensemble protects the skin against contact with BZ or other incapacitating agents dispersed as fine solid particles or in solution. Protection against ingestion would depend upon a high index of suspicion for BZ contaminated food or drink.
Toxicokinetics
BZ may be dispersed as an aerosolized collection of small particles. Alternately, it may be dissolved in a solvent such as DMSO to enhance percutaneous absorption. Bioavailability via ingestion and by inhalation of particles 1 micrometre in size approximates 80%, and 40 to 50%, respectively, of a parenterally delivered dose of BZ. Percutaneous absorption of BZ dissolved in propylene glycol yields, after a latent period of up to 24 hours, serum levels approximately 5 to 10% of those achieved with intravenous or intramuscular administration. Although inhalation of aerosolized BZ is probably the greatest risk on the battlefield, terrorists may choose to disseminate BZ in forms that provide significant opportunities for ingestion and absorption through the skin.
Following absorption, BZ is systemically distributed to most organs and biological tissues of the body. Its ability to reach synapses and neuromuscular and neuroglandular junctions throughout the body is responsible for its PNS effects, whereas its ability to cross the blood-brain barrier confers upon it the ability to cause CNS effects. Atropine and hyoscyamine both cross the placenta and can be found in small quantities in breast milk; whether this is also true for BZ is unclear.
Metabolism of BZ would be expected to occur primarily in the liver, with elimination of unchanged agent and metabolites chiefly in the urine.
Toxicity
The characteristic that makes BZ an incapacitating rather than a toxic chemical warfare agent is its high safety ratio. The amount required to produce effects is a thousand or more fold less than a fatal dose of the compound. In terms of Ct products (admittedly a sometimes problematic way of measuring dosage received after aerosol exposure), the ICt50 (the Ct product needed to produce incapacitation in 50% of an exposed group) for BZ is 112 mg·min/m³, whereas the Ld50 is estimated to be 200,000 mg·min/m³.
Toxicodynamics (mechanism of action)
The agent BZ and other anticholinergic glycolates act as competitive inhibitors of the neurotransmitter acetylcholine neurons (1) at postjunctional muscarinic receptors in cardiac and smooth muscle and in exocrine (ducted) glands and (2) at postsynaptic receptors in neurons. As the concentration of BZ at these sites increases, the proportion of receptors available for binding to acetylcholine decreases and the end organ "sees" less acetylcholine. (One way of visualizing this process is to imagine BZ coating the surface of the end organ and preventing acetylcholine from reaching its receptors.) Because BZ has little to no agonist activity with respect to acetylcholine, high concentrations of BZ essentially substitute a "dud" for acetylcholine at these sites and lead to clinical effects reflective of understimulation of end organs.
Clinical effects
Peripheral Effects:
- Mydriasis, blurred vision
Dry mouth, skin
Initially rapid heart rate declining to normal or slow heart rate over time
Possible flushing of the skin
The PNS effects of BZ are, in general, readily understood as those of understimulation of end organs and are qualitatively similar to those of atropine. Decreased stimulation of eccrine and apocrine sweat glands in the skin results in dry skin (an affected patient can be "dry as a bone") and a reduction in the ability to dissipate heat by evaporative cooling. The skin becomes warm ("hot as a hare") partly from decreased sweating and partly from compensatory cutaneous vasodilatation (the patient becomes "red as a beet," with a so-called atropine flush) as the body attempts to shunt a higher proportion of core-temperature blood as close as possible to the surface of the skin. With decreased heat loss, the core temperature itself rises.
Understimulation of other exocrine glands leads to xerostomia (dry mouth, another way in which the patient is "dry as a bone"), thirst, and decreased secretions from lacrimal, nasal, bronchial, and gastrointestinal glands.
Decreased cholinergic stimulation of pupillary sphincter muscles allows alpha-adrenergically innervated pupillary dilating muscles to act essentially unopposed, resulting in mydriasis. (In fact, the cosmetic effect of mydriasis in women who applied extracts of deadly nightshade topically to their eyes explains the name "belladonna" given to this plant.) Similar effects on cholinergic ciliary muscles produce paralysis of accommodation. Classically, the patient is described as being "blind as a bat". Other smooth muscle effects from BZ intoxication include decreased bladder tone and decreased urinary force with possibly severe bladder distention (yet another way in which the patient may be said to be "dry as a bone").
BZ typically raises the heart rate initially, but hours later, depending on the dose of BZ, the heart rate falls to normal or may become slow. Either the peripheral vagal blockade has ceased or the stimulation of the vagal nucleus has occurred.
Neither atropine nor BZ can act directly at the postjunctional nicotinic receptors found in skeletal muscle, but BZ-exposed patients nonetheless exhibit muscle weakness. This weakness, along with incoordination, heightened stretch reflexes, and ataxia, is probably due to the effects of BZ at CNS sites.
The PNS effects of BZ are essentially side effects that are useful in diagnosis, but incidental to the CNS effects for which the incapacitating agents were developed. These CNS effects include a dose-dependent decrease in the level of consciousness, beginning with drowsiness and progressing through sedation to stupor and coma. The patient is often disoriented to time and place. Disturbances in judgment and insight appear. The patient may abandon socially imposed restraints and resort to vulgar and inappropriate behavior. Perceptual clues may no longer be readily interpretable, and the patient is easily distracted and may have memory loss, most notably short-term memory. In the face of these deficits, the patient still tries to make sense of his environment and will not hesitate to make up answers on the spot to questions that confuse him. Speech becomes slurred and often senseless, and loss of inflection produces a flat, monotonous voice. References become concrete and semiautomatic with colloquialisms, clichés, profanity, and perseveration. Handwriting also deteriorates. Semiautomatic behavior may also include disrobing (perhaps partly because of increased body temperature), mumbling, and phantom behaviors such as constant picking, plucking, or grasping motions ("woolgathering" or carphology).
It should be noted that BZ was supposedly administered to soldiers during the Vietnam War in the film Jacob's Ladder, but the specified effects are not accurate and possibly exaggerated. It has not been proven that BZ sends people exposed to it in a homicidal frenzy, as the film suggests.
Central effects
- Disturbances in level of consciousness
Misperceptions and difficulty in interpretation (delusions, hallucinations)
Poor judgment and insight (denial of illness)
Short attention span, distractibility, impaired memory (particularly recent)
Slurred speech, perseveration
Disorientation
Ataxia
Variability (quiet/restless)
Central nervous system mediated perceptual disturbances in BZ poisoning include both illusions (misidentification of real objects) and hallucinations (the perception of objects or attributes that have no objective reality). (Although the phrase "mad as a hatter" refers to poisoning from mercury formerly used by hatters on felt, it can just as well serve as a reminder of CNS effects from anticholinergics.) Hallucinations resulting from anticholinergics such as BZ tend to be realistic, distinct, easily identifiable (often commonly encountered objects or persons), panoramic, and difficult to distinguish from reality. They also have the tendency to decrease in size during the course of the intoxication. This is in contrast to the typically vague, ineffable, and transcendent-appearing hallucinations induced by psychedelics such as LSD.
Another prominent CNS finding in BZ poisoning is behavioral lability, with patients swinging back and forth between quiet confusion and self-absorption in hallucinations, to frank combativeness. Moreover, as other symptoms begin to resolve, intermittent paranoia may be seen. Automatic behaviors common during resolution include the crawling or climbing motions called "progresso obstinato" in old descriptions of dementia.
BZ produces effects not just in individuals, but also in groups. Sharing of illusions and hallucinations (folie à deux, folie en famille, and "mass hysteria") is exemplified by two BZ-intoxicated individuals who would take turns smoking an imaginary cigarette clearly visible to both of them but to no one else. [Clarification] When one observed subject mumbled, "Gotta cigarette?" His delirious companion held out an invisible pack, he followed with, "S'okay, don't wanna take your last one." In another test it was reported two victims of BZ played tennis with imaginary rackets.
Time course of effects
Clinical effects from ingestion or inhalation of BZ appear after an asymptomatic or latent period that may be as little as 30 minutes, or as long as 20 hours; the usual range is 0.5 to 4 hours, with a mean of 2 hours. However, effects may not appear up to 36 hours after skin exposure to BZ.
Once effects appear, their duration is typically 72 to 96 hours and are dose-dependent. Following an ICt50 of BZ, severe effects may last 36 hours, but mild effects may persist for an additional day.
The clinical course from BZ poisoning can be divided into the following four stages:
- Onset or induction (zero to four hours after exposure), characterized by parasympathetic blockade and mild CNS effects.
- Second phase (4 to 20 hours after exposure), characterized by stupor with ataxia and hyperthermia.
- Third phase (20 to 96 hours after exposure), in which full-blown delirium is seen but often fluctuates from moment to moment.
- Fourth phase, or resolution, characterized by paranoia, deep sleep, reawakening, crawling or climbing automatisms, and eventual reorientation.
Differential diagnosis
The differential diagnosis for irrational and confused patients is a long one and includes anxiety reactions as well as intoxication with a variety of agents, to include hallucinogenic indoles (such as LSD), cannabinoids (such as the delta-9-tetrahydrocannabinol in marijuana), lead, barbiturates, and bromides. All of these conditions can lead to restlessness, lightheadedness (with associated vertigo and ataxia), confusion, and erratic behavior with or without vomiting. Clues that specifically point to BZ or a related compound are the combination of anticholinergic PNS effects ("dry as a bone," "hot as a hare," "red as a beet," and "blind as a bat") with the CNS effects ("mad as a hatter") of slurred and monotonous speech, automatic behavior (perseveration, disrobing, and phantom behaviors (such as "woolgathering"), and vivid, realistic, describable hallucinations (decreasing in size over time) in a patient slipping into and out of delirium.
Signs and symptoms
- Restlessness
- Dizziness or giddiness
- Failure to obey orders
- Confusion
- Erratic behavior
- Stumbling or staggering
- Drymouth (cottonmouth)
- Tachycardia at rest
- Elevated temperature
- Flushing of face
- Blurred vision
- Pupillary dilation
- Slurred or nonsensical speech
- Hallucinations
- Disrobing
- Mumbling
- Stupor and coma.
- Inappropriate smiling or laughter
- Irrational fear
- Distractability
- Difficulty expressing self
- Elevated blood pressure
- Stomach cramps and vomiting
- Euphoric, relaxed, unconcerned attitude
- Hypotension and/or dizziness on sudden standing
- Tremor
- Clinging or pleading
- Seemingly reasonless crying
- Decrease in disturbance with reassurance
Anticholinergics
- Indoles (Schizophrenic psychosis may mimic in some
respects.)
Cannabinols
Anxiety reaction
Atropine intoxication from MARK I autoinjector use in a patient not exposed to nerve agents may create similar PNS effects to those seen in BZ intoxication. However, marked confusion from atropine is not normally seen until a total of six or seven autoinjectors have been given (in a hot, dehydrated, or battle-stressed individual, less atropine would probably suffice). Circumstantial evidence may be helpful in this situation. Heat stroke may also generate hot, dry, and confused or stuporous casualties and needs to be considered in the differential diagnosis. Patients with anxiety reactions are usually oriented to time, place, and person but may be trembling, crying, or otherwise panicked. The classic picture of unconcern or "la belle indifférence" may characterize a patient with a conversion reaction, but these patients are also likely to be oriented and lack the anticholinergic PNS signs of BZ poisoning.
Medical management
The admonition to protect oneself first may be difficult when dealing with any intoxication involving a latent period, since initially asymptomatic exposure to health care providers may already have occurred during the same time frame in which patients were exposed. Protection of medical staff from already absorbed and systemically distributed BZ in a patient is not needed.
General supportive management of the patient includes decontamination of skin and clothing (ineffective for already absorbed agent but useful in preventing further absorption of any agent still in contact with the patient), confiscation of weapons and related items from the patient, and observation. Physical restraint may be required in moderately to severely affected patients. The greatest risks to the patient's life are (1) injuries from his or her own erratic behavior (or from the behavior of similarly intoxicated patients) and (2) hyperthermia, especially in patients who are in hot or humid environments or are dehydrated from overexertion or insufficient water intake. A severely exposed patient might be comatose with serious cardiac arrhythmias and electrolyte disturbances. Management of heat stress assumes a high priority in these patients. Because of the prolonged time course in BZ poisoning, consideration should always be given to evacuation to a higher echelon of care.
As a competitive inhibitor of acetylcholine, BZ effectively decreases the amount of acetylcholine "seen" by postsynaptic and postjunctional receptors throughout the body. Specific antidotal therapy in BZ poisoning is therefore geared toward raising the concentration of acetylcholine in these synapses and junctions. Any compound that causes a rise in acetylcholine concentration can potentially overcome BZ-induced inhibition and restore normal functioning; even the nerve agent VX has been shown to be effective when given under carefully controlled conditions. The specific antidote of choice in BZ poisoning is the carbamate anticholinesterase physostigmine (eserine; Antilirium®), which temporarily raises acetylcholine concentrations by binding reversibly to anticholinesterase on the postsynaptic or postjunctional membrane. Physostigmine is similar in many ways to pyridostigmine and is equally effective when used as a pre-exposure antidotal enhancer ("pretreatment") in individuals at high risk for subsequently encountering soman. However, physostigmine is not used for this purpose because the doses required cause vomiting through CNS mechanisms. In the case of BZ poisoning, a nonpolar compound such as physostigmine is used specifically because penetration into the brain is required in those individuals who already have CNS effects from BZ.
In BZ-intoxicated patients, physostigmine is minimally effective during the first four hours after exposure but is very effective after four hours. Oral dosing generally requires one and a half times the amount of antidote as does IM or IV administration. However, effects from a single intramuscular injection of physostigmine last only about 60 minutes, necessitating frequent re-dosing. It must be emphasized that physostigmine does not shorten the clinical course of BZ poisoning and that relapses will occur if treatment is discontinued prematurely. The temptation to substitute a slow intravenous infusion for intramuscular injections should be tempered by the awareness that IV infusion may lead to nerve-agent-like bradycardia, and too rapid infusion might cause arrhythmias, excessive secretions (to the point of compromising air exchange), and convulsions. Moreover, the sodium bisulfite in commercially available preparations of physostigmine may cause life-threatening allergic responses.
Suggested dosages for physostigmine in the treatment of BZ poisoning follow:
Test dose: If the diagnosis is in doubt, a dose of 1 mg might be given. If a slight improvement occurs, routine dosing should be given.
Routine dosing: Doses of about 45 µg/kg for adults have been recommended. This might be modified by the response. A mental status examination should be done every hour and the dose and time interval of dosing should be modified according to whether the mental status is improved or not. As the patient improves, the dosage requirement will decrease.
Routes of administration:
- IM: 45 µg/kg in adults (20 µg/kg in children)
- IV: 30 µg/kg slowly (1 mg/min)
- PO: 60 µg/kg if patient is cooperative (because of bitter taste, consider diluting in juice)
For each route, titrate about every 60 minutes to mental status.
History and toxicity of physostigmine
The antagonism between physostigmine (the elixir of calabar bean) and atropine (tincture of belladonna) was first reported in 1864 by a physician who successfully treated prisoners who had become delirious after drinking tincture of belladonna. Physicians did not notice this report until the 1950s when atropine coma (in which 50 mg or so of atropine were given to certain psychiatric patients) was successfully treated with physostigmine after the "therapeutic benefit" had been attained. Again, this went unnoticed until a controlled study, reported in 1967, indicated that anticholinergic intoxication could be successfully, albeit transiently, reversed by physostigmine.
A recent textbook of emergency medicine stated that physostigmine should be used only as "a last resort." It would seem that when a patient needs "last resort" care is the absolute wrong time to administer a potent cholinesterase inhibitor.
The administration of physostigmine by the IV route in a delirious but conscious and otherwise healthy patient is not without peril. It is sometimes difficult to keep a delirious patient quiet long enough to administer the drug (at 1 mg/min is the marketed solution of 1 mg/ml). Even if administered correctly (very slowly), the heart rate may decline from 110 to 45 beat/min over a period of 1 to 2 minutes. The difference in the onset of the effects after IM and IV administration of physostigmine is a matter of only several minutes. Since its use is rarely lifesaving, this slight difference in time of response is inconsequential.
Physostigmine is a safe and effective antidote if used properly. In a conscious and delirious patient it will produce very effective but transient reversal of both the peripheral and central effects of cholinergic blocking compounds. Its use by the IV route is not without hazards. It absolutely should NOT be used in a patient with cardiorespiratory compromise, hypoxia, or acid-base imbalance with a history of seizure disorders or arrhythmias.
Triage
An immediate casualty (possible but unlikely) would be one with cardiorespiratory compromise or severe hyperthermia. Immediate attention to ventilation, hemodynamic status, and temperature control could be lifesaving. Because of its dangers in a hypoxic or hemodynamically challenged patient, physostigmine should be considered a second-line management option to be used only if adequate attention can simultaneously be given to temperature and other vital signs.
The delayed casualty would present with pronounced or worsening anticholinergic signs. Physostigmine should definitely be considered in this kind of patient.
A minimal casualty from a strictly medical standpoint might have mild PNS or CNS anticholinergic effects. Given the time course of BZ intoxication, however, these patients should not be considered able to manage themselves or capable of routine return to duty and should be relieved of their weapons, observed, and, if the holding capacity at the current echelon is exceeded, evacuated.
An expectant casualty (also possible but unlikely) would have severe cardiorespiratory compromise in a situation in which treatment or evacuation resources are too limited to allow the necessary attention to be directed to him or her.
Return to duty
Given the time course of the intoxication, early return to duty is probably not a realistic possibility for the majority of casualties who may require observation and management for several days at the least.
The original version of this page is taken from the public domain source at [2]
External links
- Erowid - BZ Vault
- Tear Gases and Chemical Agents - Agent BZ
- eMedicine - Incapacitating Agents: 3-Quinuclidinyl Benzilate
- Abuse of BZ by Insurgents in Iraq
- Center for Disease Control - BZ Incapacitating Agent
